While AORC occurs in children, it is difficult to acquire population data on them, so most of the estimates presented in this report are for adults unless otherwise noted.
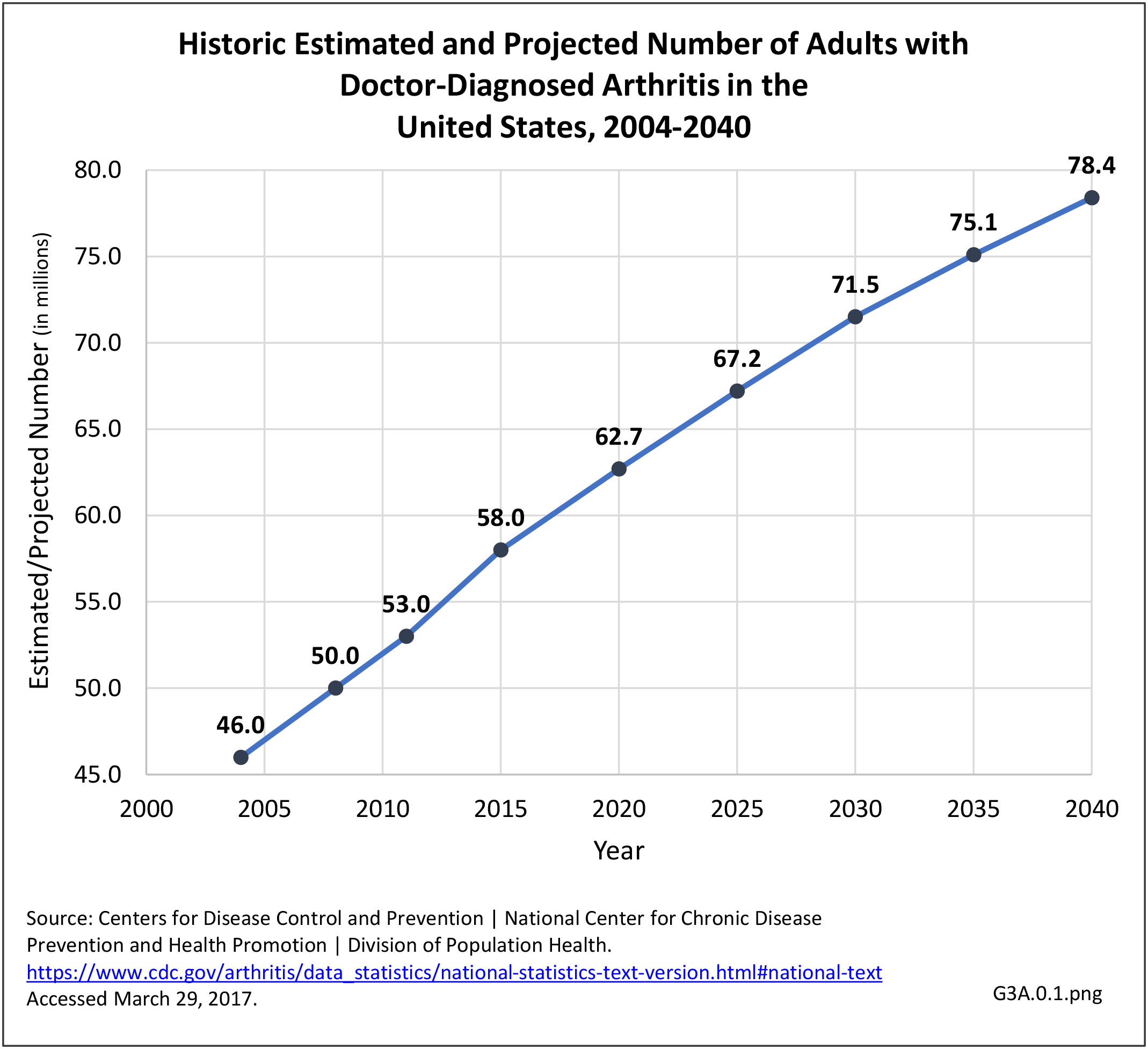
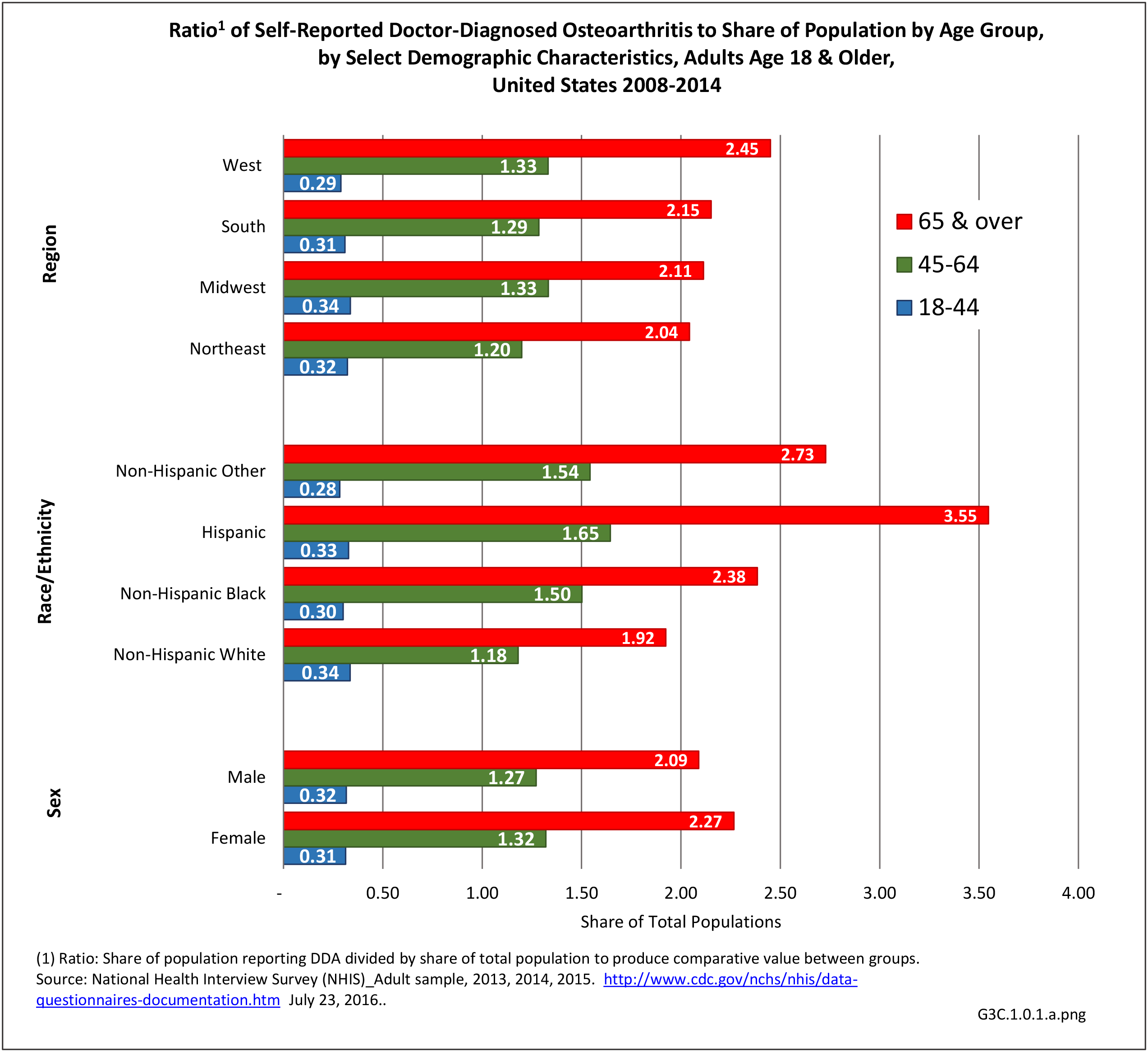
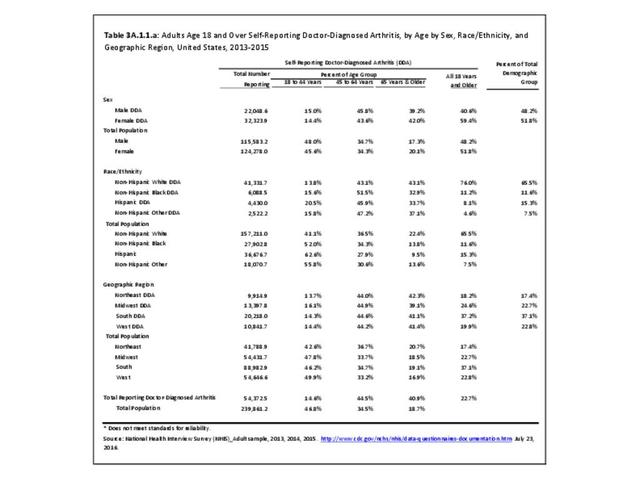
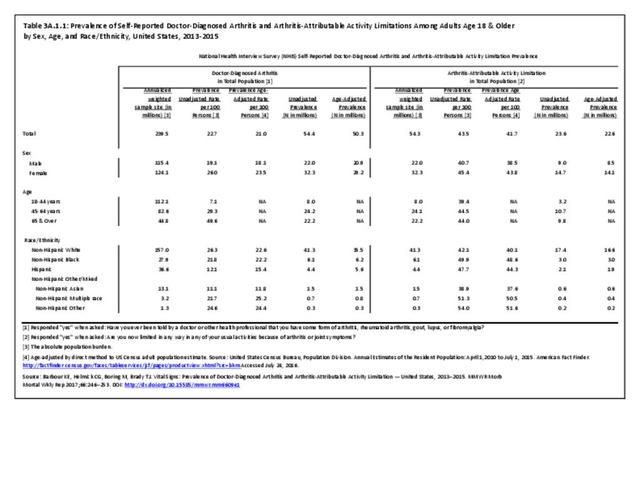
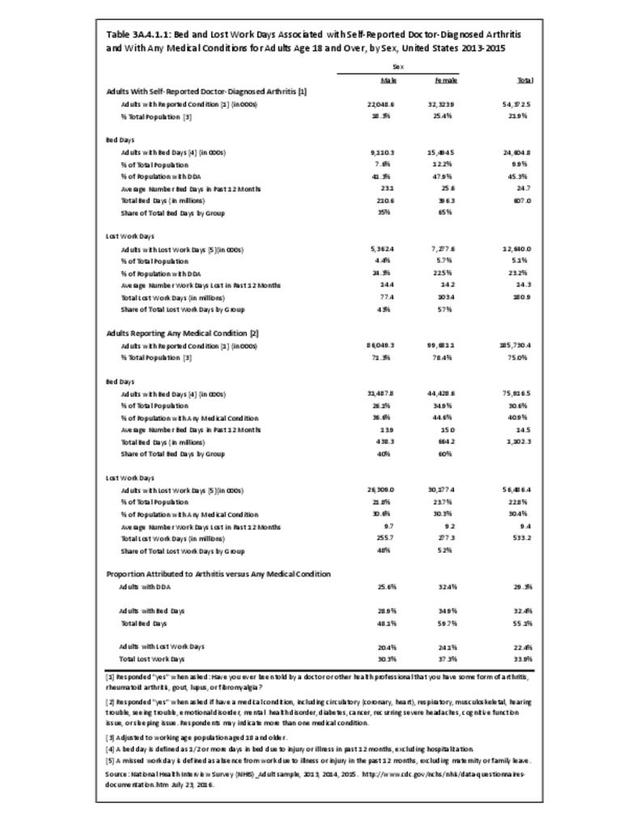
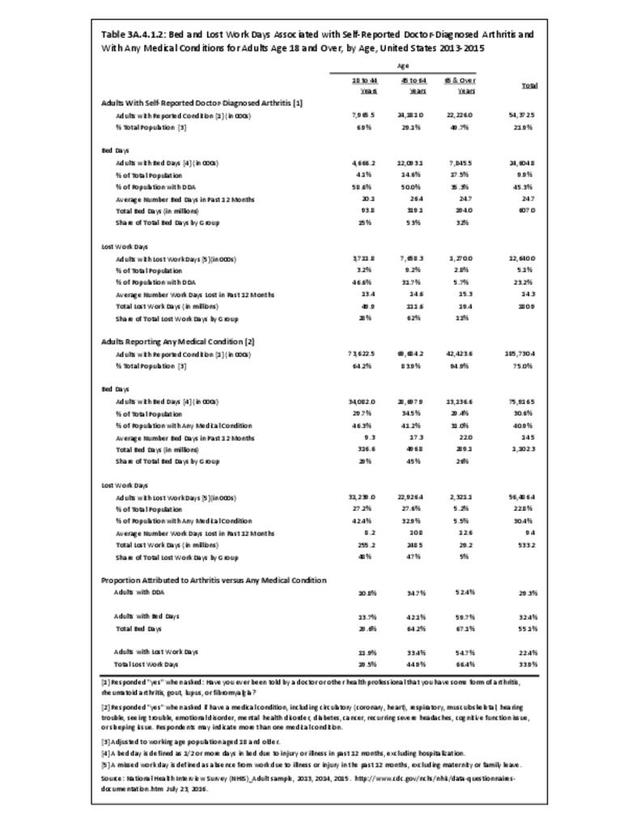
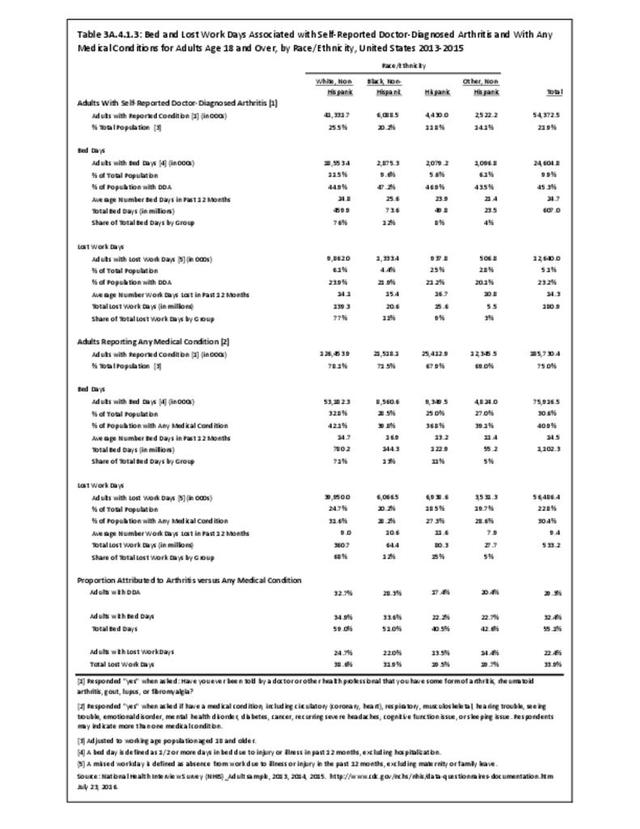
In the general population, prevalence is better estimated by DDA than AORC. For the years 2013-2015, DDA affected an unadjusted average of 54.4 million adults, or 23 in 100 adults.1 Estimates show the typical distribution of higher prevalence among females and older adults, and lower prevalence among Hispanics and Asians. Absolute estimates show that most of these adults (59%, or 32.2 million) are of working age (younger than age 65).1 (Reference Table 3A.1.1 PDF CSV)

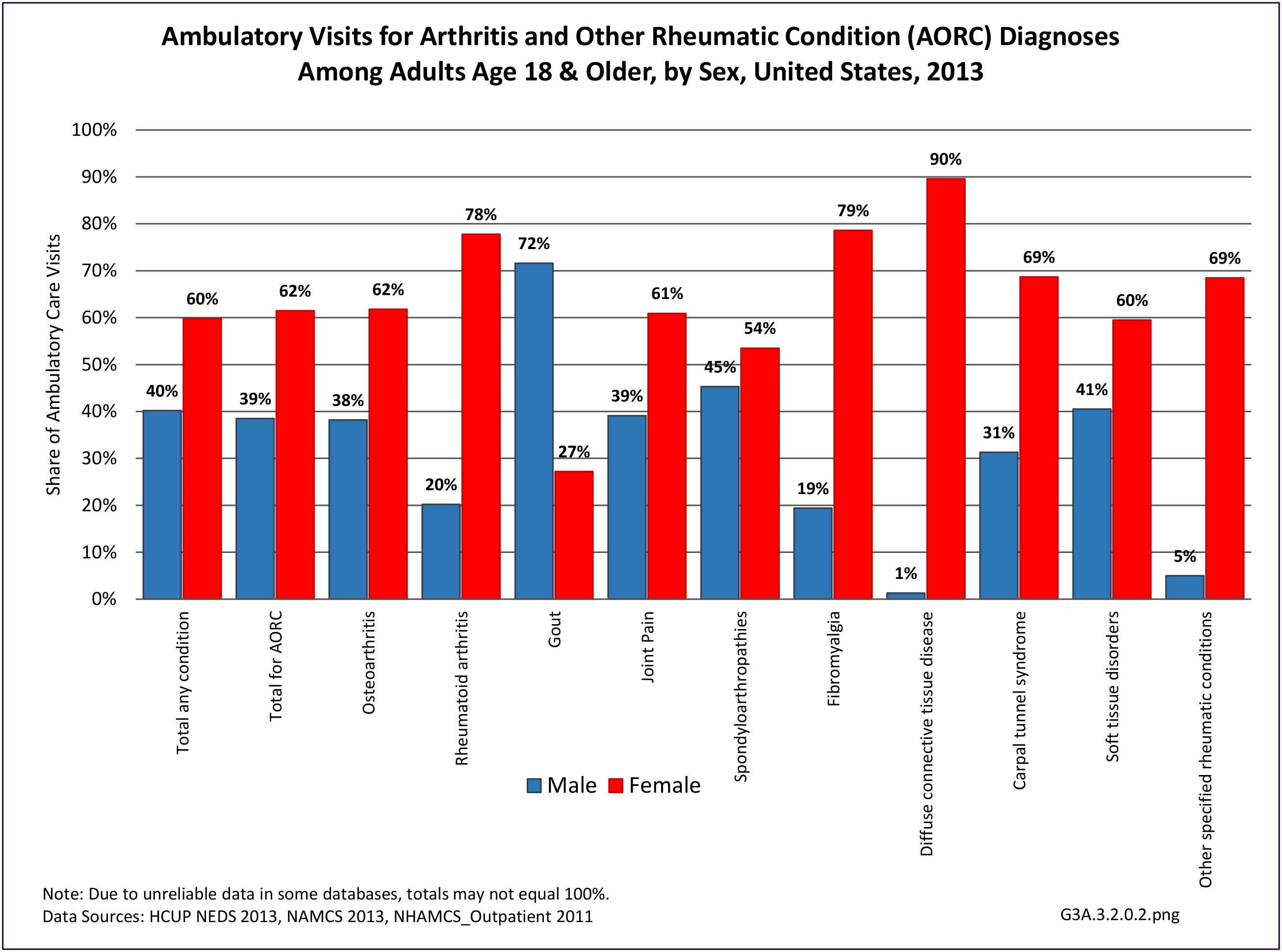
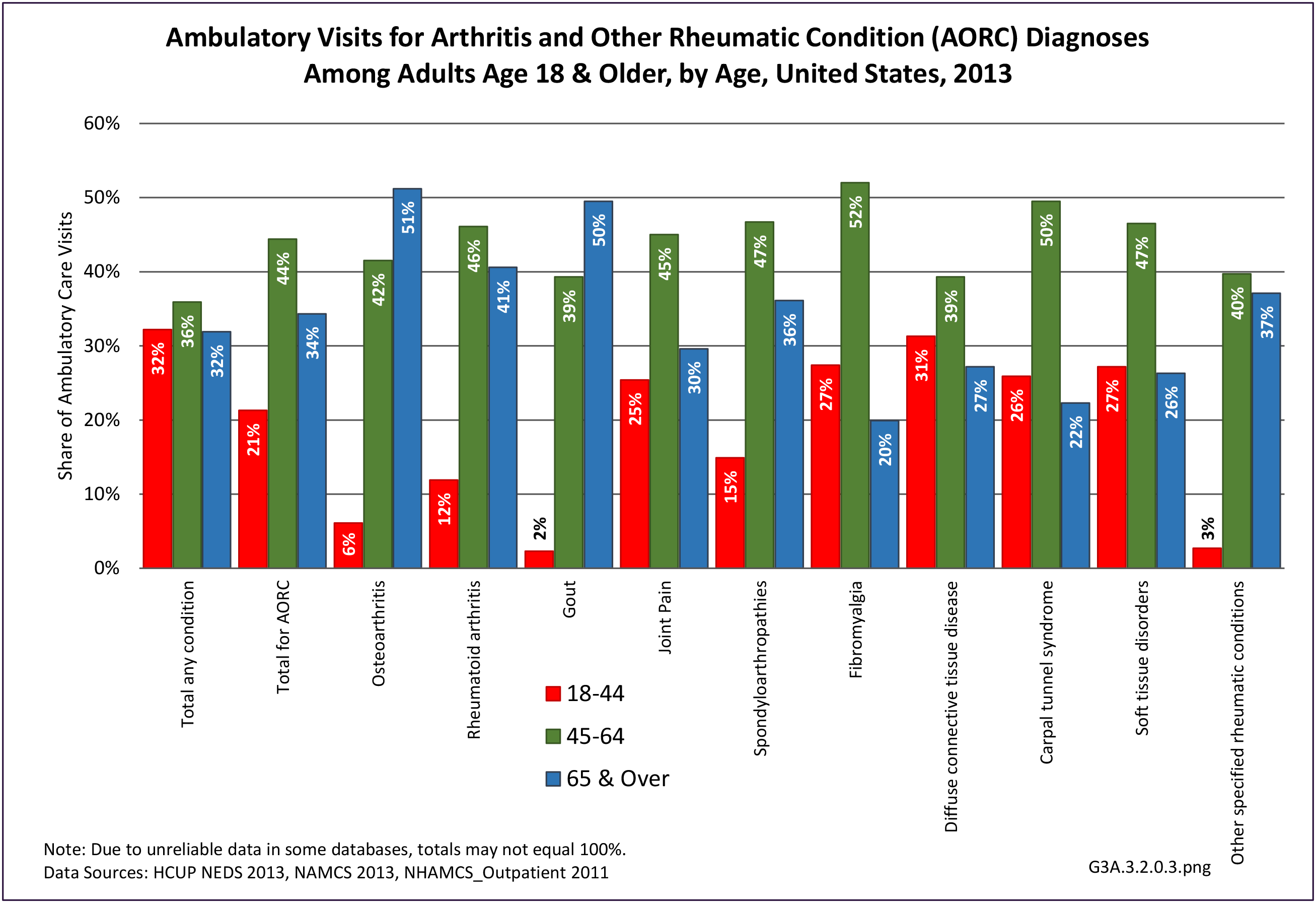
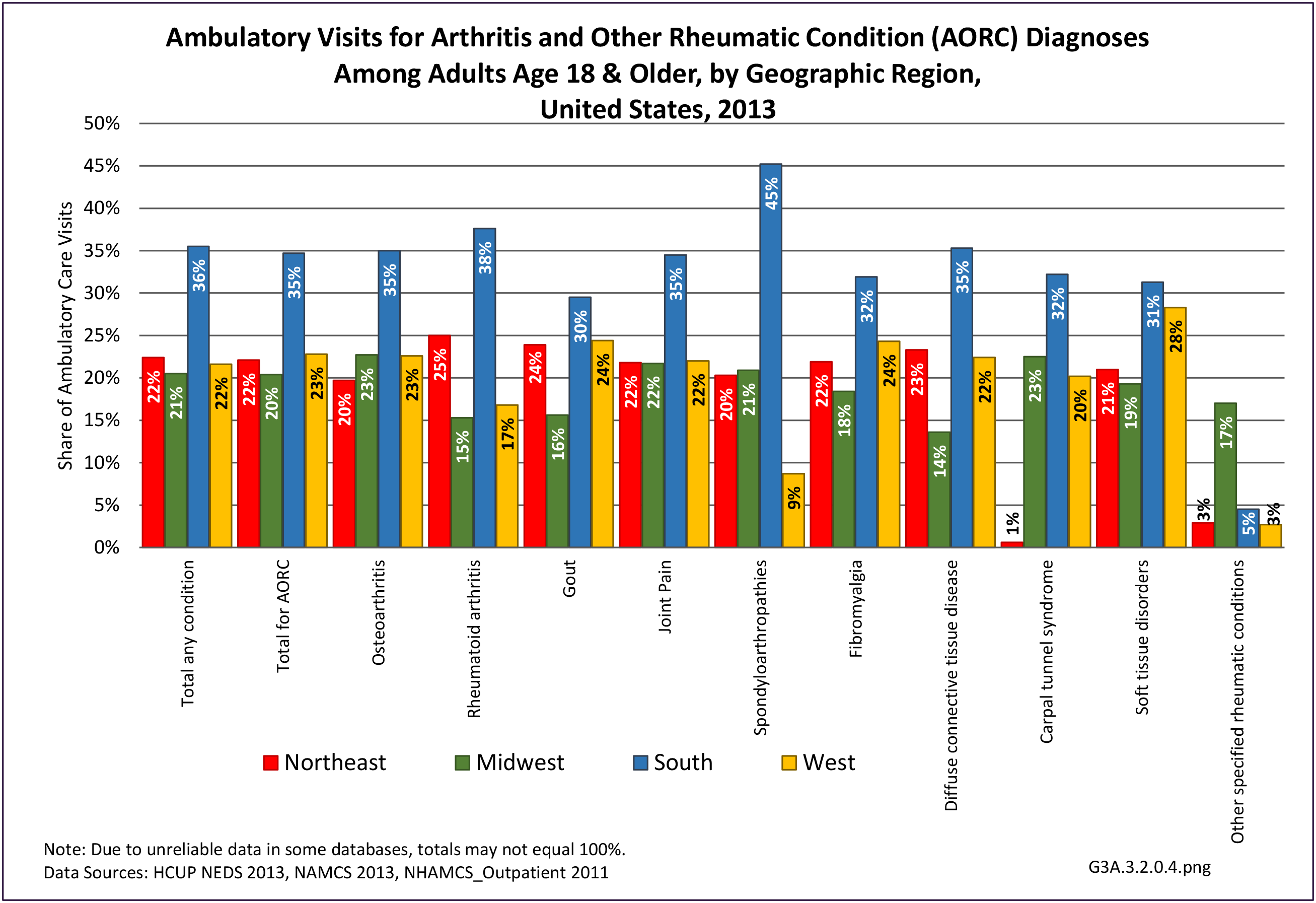
Specific types of AORC
Clinical data are required to provide some measure of validity for estimating the prevalence of specific types of arthritis because many people are not sure what type of arthritis they have. Data from the National Arthritis Data Workgroup provided 2005 national prevalence estimates for some of the ten specific types of arthritis used in later tables.2,3 Respondents could have reported more than one type.
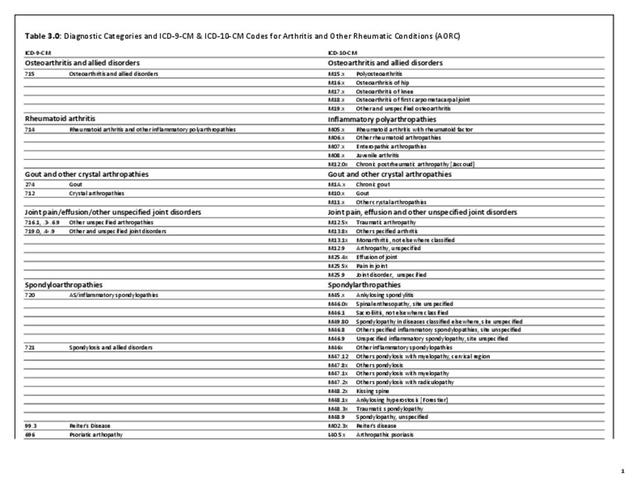
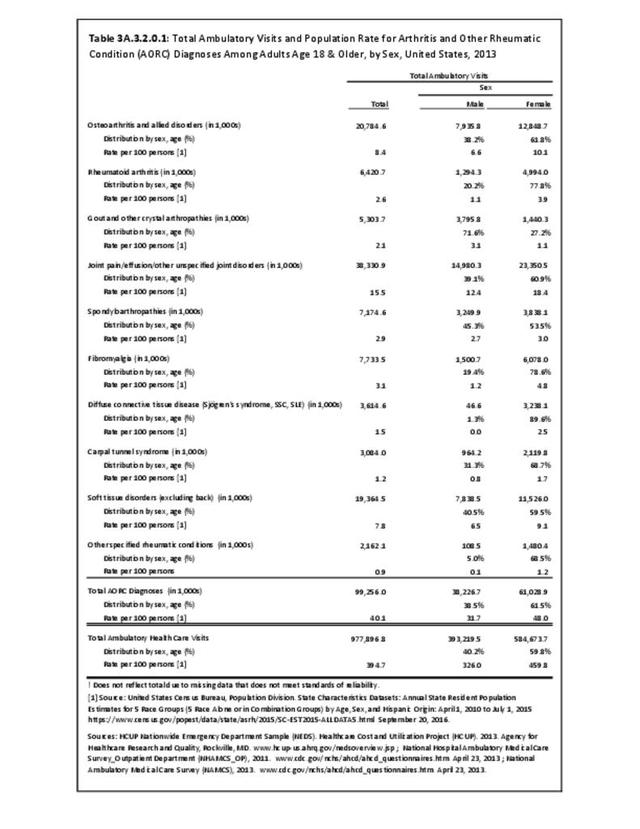
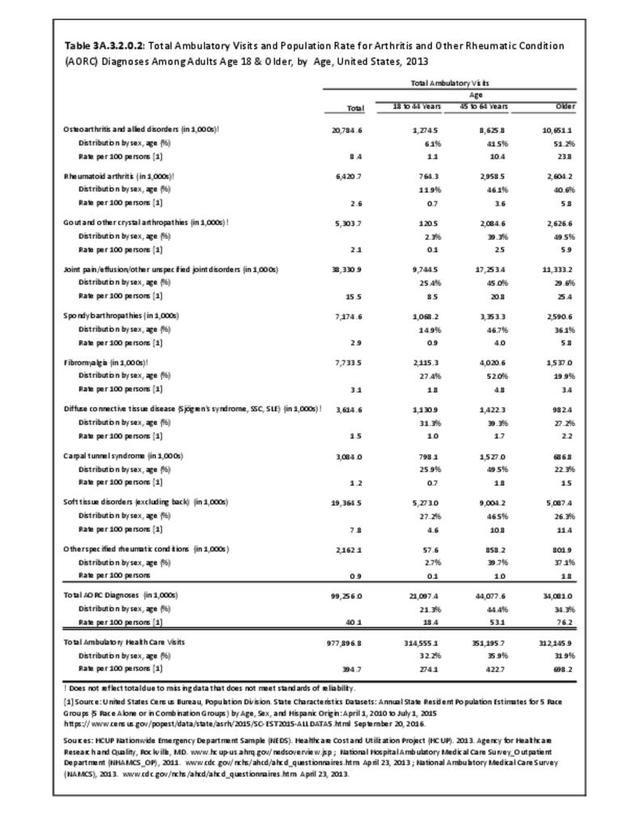
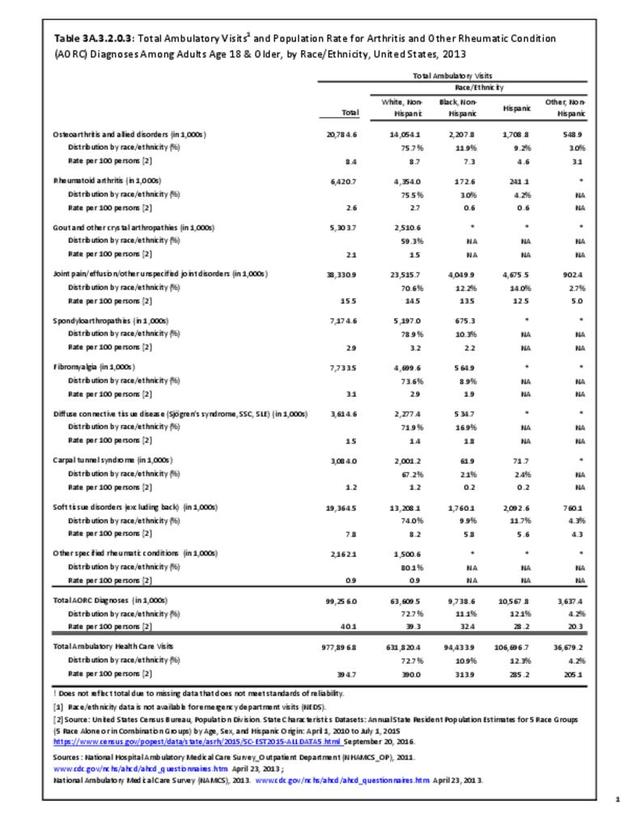
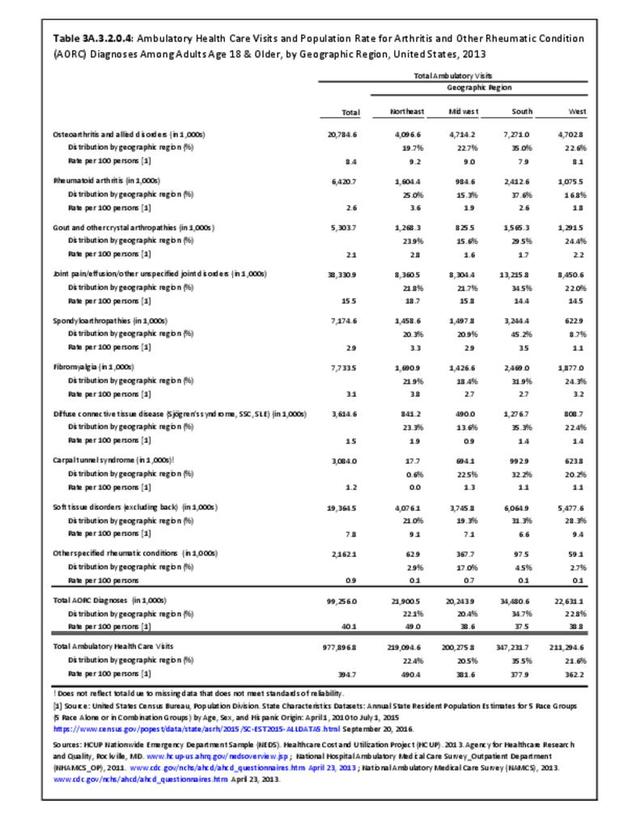
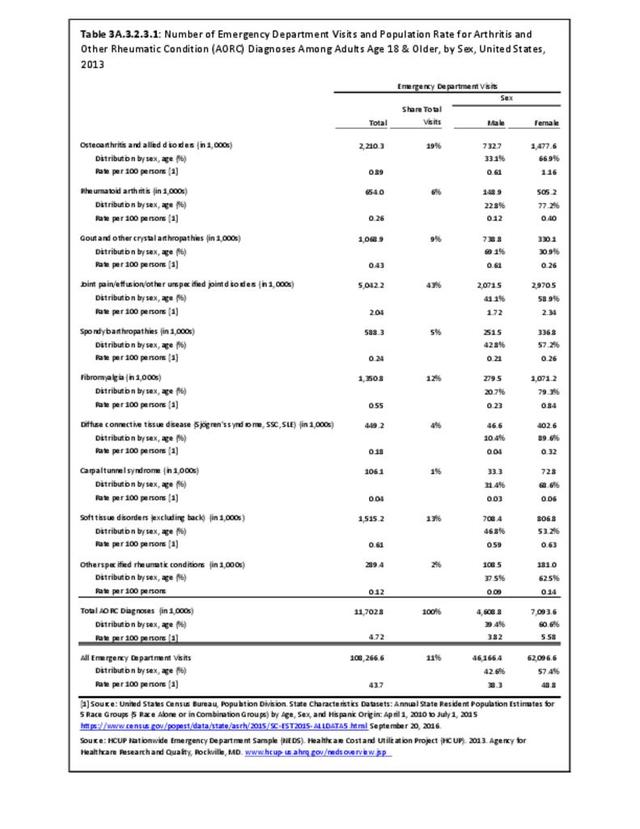
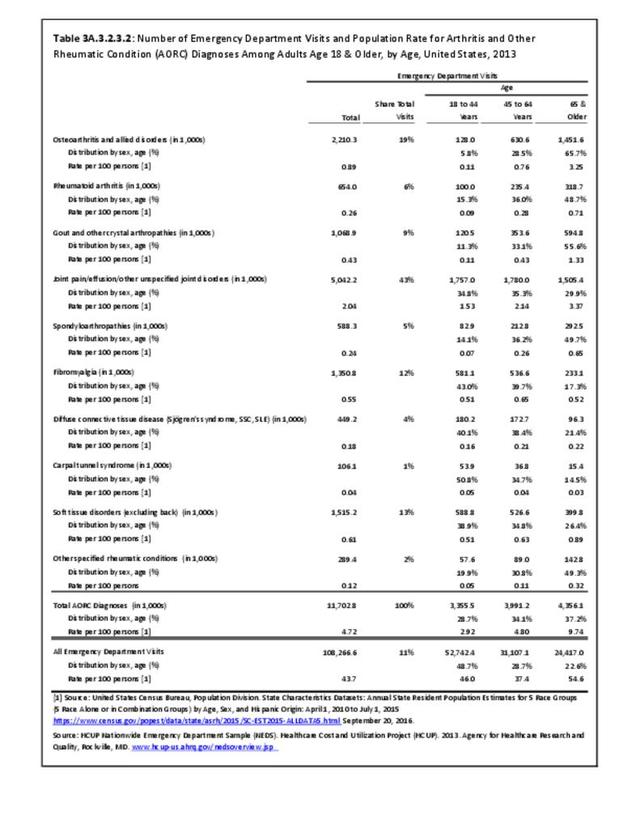
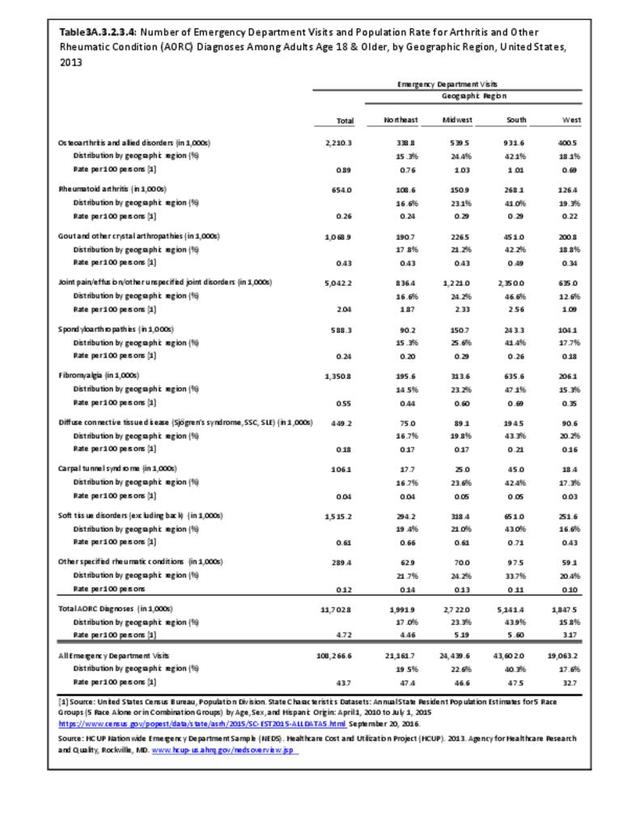
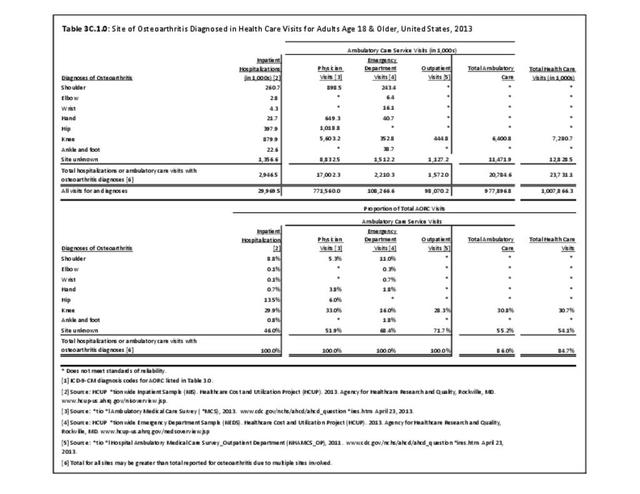
Osteoarthritis: Osteoarthritis (OA) is the most common type of arthritis, characterized by progressive damage to cartilage and other joint tissues. Joint injury is a risk factor for OA, but most cases occur without a specific history of injury. Obesity is a risk factor for knee OA, and to a lesser extent for hip and hand OA. Clinical OA was estimated to affect 26.9 million in 20053 and over 30 million for 2008-2011.4 The joints most affected with radiographic OA and symptomatic OA were hands, knees, and hips.3
Rheumatoid arthritis: Rheumatoid arthritis (RA) is the prototypical inflammatory arthritis. It is a chronic autoimmune disease that causes pain, aching, stiffness, and swelling in multiple joints, especially the hands, in a symmetrical fashion. In 2005, RA was estimated to affect 1.3 million adults.2
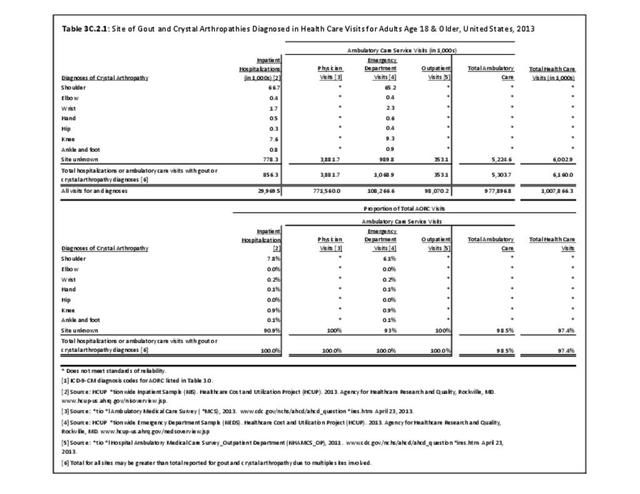
Gout and other crystal arthropathies: Gout is a recurrent inflammatory arthritis that occurs when excess uric acid collects in the body. Gout has been recognized for centuries and often affects the big toe. In 2005, an estimated 6.1 million adults reported having gout at some time, with 3.0 million affected in the past year.3 More recent studies of self-reported gout and hospitalizations show the prevalence of gout increasing in the last two decades.5,6
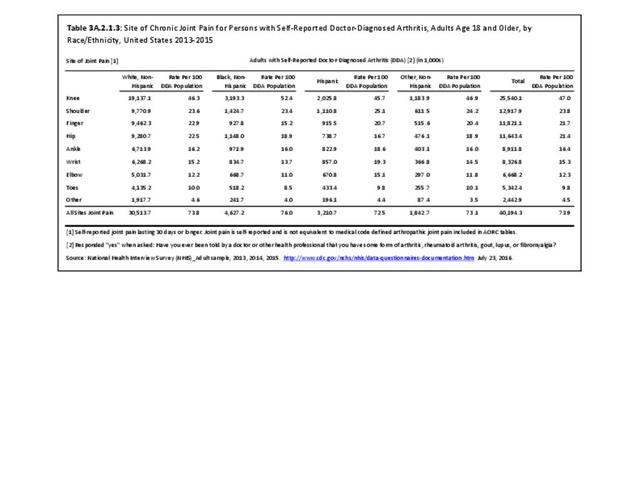
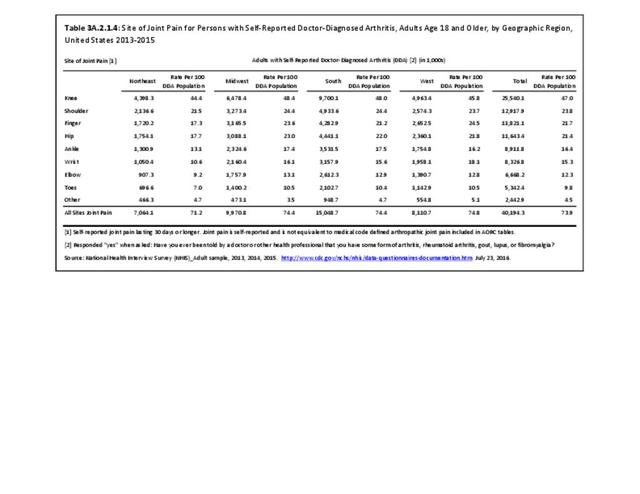
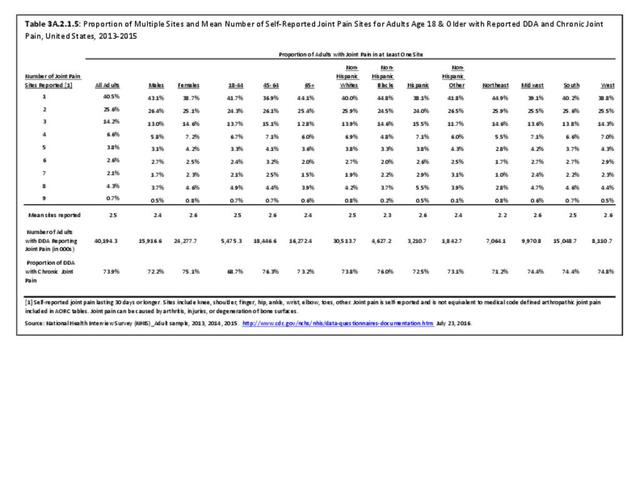
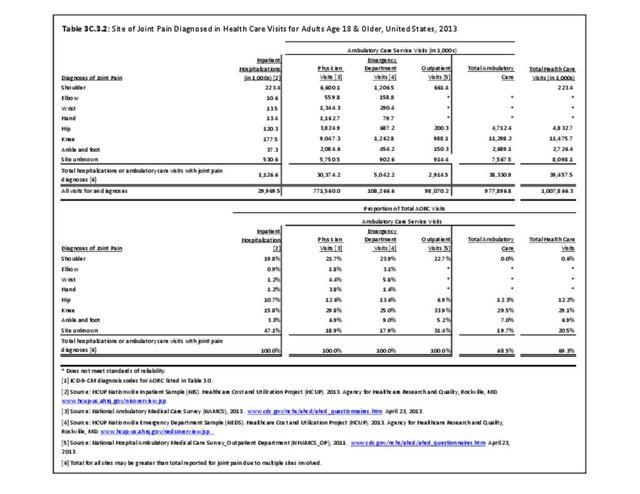
Joint pain/effusion/other unspecified joint disorders: Joint pain can result from several causes, including inflammation, degeneration, crystal deposition, infection, and trauma. Joint pain is often accompanied by swelling and effusion. A joint effusion is the presence of increased intra-articular fluid within the synovial compartment of a joint. Determining the cause of joint pain is primary to treatment.
Spondylarthropathies: Spondylarthropathies (or spondylarthritides) are a family of diseases that includes ankylosing spondylitis, reactive arthritis, psoriatic arthritis, enteropathic arthritis (associated with ulcerative colitis or Crohn’s disease), juvenile spondylarthritis, and undifferentiated spondylarthritis. In 2005, spondylarthropathies affected an estimated 639,000 to 2.4 million adults ages 25 and older.2
Fibromyalgia: Fibromyalgia (FM) is a syndrome of widespread pain and tenderness. The diagnosis is difficult to make, so relevant prevalence data are hard to come by. In 2005, FM was estimated to affect around 5 million adults.3 A more recent estimate by the National Fibromyalgia Association puts the estimate at 10 million people in the US, with 75%-90% of the affected adult women. However, due to the difficulty in diagnosing fibromyalgia and the potential for including other causes of pain, this estimate should be used with caution.7
Diffuse connective tissue diseases include the next four diseases.
Systemic lupus erythematosus: Systemic lupus erythematosus (SLE) is the prototypical autoimmune disease in which the body’s immune system can attack many body systems, especially the skin, kidneys, and joints. In 2005, definite and suspected SLE was conservatively estimated to affect 322,000.2 Population-based registries have provided more recent estimates for various racial/ethnic groups.8,9,10
Systemic Sclerosis: Systemic sclerosis (SSc), or scleroderma, is an autoimmune disease that primarily affects the skin, but can affect any organ system. In 2005, SSc affected an estimated 49,000 adults.2
Primary Sjögren’s Syndrome: Primary Sjögren’s Syndrome (SS) is a syndrome of dry eyes, dry mouth, and arthritis. Secondary SS can occur in association with other rheumatologic diseases such as rheumatoid arthritis and lupus. Prevalence data are very limited. In 2005, an estimated 0.4 to 3.1 million adults had SS.2
Polymyalgia rheumatica and giant cell (temporal) arteritis: Polymyalgia rheumatica (PMR) is a syndrome of sudden aching and stiffness in older adults that responds to treatment with anti-inflammatory medications (e.g., corticosteroids). Giant cell arteritis (GCA), which often occurs with PMR, is a type of vasculitis that affects medium-size arteries and results in headache, vision loss, and other symptoms. In 2005, PMR was estimated to affect 711,000 adults;3 a more recent analysis from the same data source found that the incidence of PMR had increased slightly with mortality not unlike the general population,11 suggesting that prevalence may have increased slightly as well. In 2005, GCA was estimated to affect 228,000 adults.4
Carpal tunnel syndrome: Carpal tunnel syndrome (CTS) occurs when the median nerve becomes compressed at the wrist and causes numbness, pain, or weakness in part of the hand. Thickened tendons and other rheumatic conditions are a common cause. General population prevalence has been reported between 1% and 5%.12
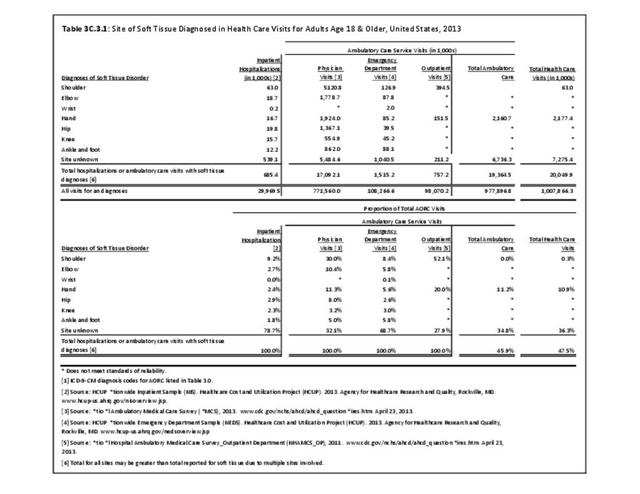
Soft tissue disorders (excluding back): These are a variety of problems of the tendons, bursa, muscle, ligaments, and fascia that cause pain and dysfunction. Prevalence of soft tissue disorders is difficult to determine due to the variety of conditions included.
Other specific rheumatic conditions: These are other conditions that the National Arthritis Data Workgrop considered to be rheumatic conditions.
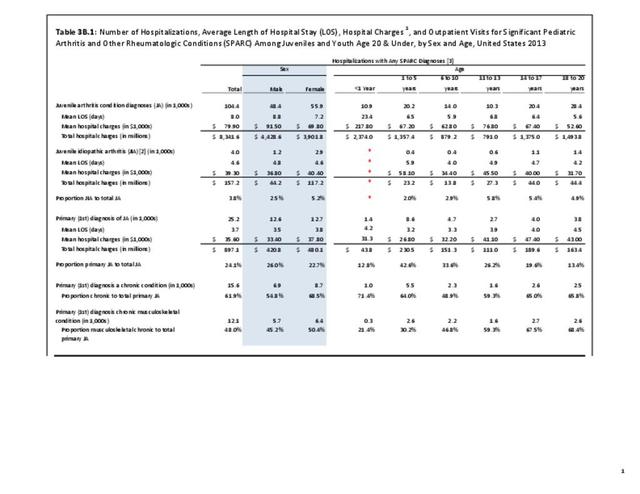
Juvenile arthritis: Arthritis and other rheumatic conditions are relatively uncommon in children, although they can be particularly severe when they do occur. One estimate using significant pediatric arthritis and other rheumatologic conditions (SPARC) codes put the average annual prevalence at 103,000 children for the years 2001-2004 for the combined codes for rheumatoid arthritis and other inflammatory polyarthropathies, allergic purpura, arthropathy associated with infections, other and unspecified arthropathies, polyarteritis nodosa and allied conditions, and rarer inflammatory conditions.The prevalence for all SPARC codes, including synovitis and myalgia, was 294,000.13 A more in-depth discussion can be found in the Juvenile Arthritis (click HERE to open new page) section later in this document.
- 1. a. b. Barbour KE, Helmick CG, Boring M, Brady TJ. Prevalence of doctor-diagnosed arthritis and arthritis-attributable activity limitation—United States, 2013-2015. MMWR 2017;66(9):246-253.
- 2. a. b. c. d. e. f. Helmick CG, Felson DT, Lawrence RC, et al., for the National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis Rheum 2008;58(1):15-25.
- 3. a. b. c. d. e. f. Lawrence RC, Felson DT, Helmick CG, et al., for the National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis Rheum 2008;58(1):26-35.
- 4. a. b. Cisternas MG, Murphy L, Sacks J, et al., Alternative methods for defining osteoarthritis and the impact on estimating prevalence in a US population-based survey. Arthritis Care Res 2016;68(5):574-580.
- 5. Lim SY, Lu N, Oza A, et al., Trends in gout and rheumatoid arthritis hospitalizations in the United States, 1993-2011. JAMA. 2016:315(21);2345-2346.
- 6. Roddy E, Choi H. Epidemiology of gout. Rheum Dis Clin North Am. 2014:40(2);155-175. Doi: 10.1016/j.rdc.2014.01.001.
- 7. National Fibromyalgia Association. http://www.fmaware.org/about-fibromyalgia/prevalence/ Accessed April 18, 2017.
- 8. Lim SS, Bayakly AR, Helmick CG, et al., The incidence and prevalence of systemic lupus erythematosus, 2002-2004: The Georgia Lupus Registry. Arthritis Rheum 2014;66(2):357-368. DOI 10.1002/art.38329.
- 9. Somers EC, Marder W, Cagnoli P, et al., Population-based incidence and prevalence of systemic lupus erythematosus: The Michigan Lupus Epidemiology & Surveillance Program. Arthritis Rheum 2014;66(2):369-378. DOI 10.1002/art.38328.
- 10. Ferucci ED, Johnston JM, Gaddy JR, et al., Prevalence and incidence of systemic lupus erythematosus in a population-based registry of American Indian and Alaska Native people, 2007-2009. Arthritis Rheum 2014;66(9):2494-2502. DOI 10.1002/art.38720.
- 11. Raheel S, Shbeeb I, Crowson CS, Matteson EL. Epidemiology of polymyalgia rheumatica 2000-2014 and examination of incidence and survival trends over 45 years: A population-based study. Arthritis Care Res (Hoboken). 2016 Oct 21. doi: 10.1002/acr.23132. [Epub ahead of print] PMID: 27768840.
- 12. Dale AM, Harris-Adamson C, Rempel D. et al. Prevalence and incidence of carpal tunnel syndrome in US working populations: Pooled analysis of six prospective studies. Scand J Work Environ Health. 2013 Sep 1; 39(5): 495–505. doi: 10.5271/sjweh.3351.
- 13. Sacks JJ, Helmick CG, Luo Y-H, et al., Prevalence of and annual ambulatory healthcare visits for pediatric arthritis and other rheumatologic conditions in the US in 2001–2004. Arthritis Rheum (Arthritis Care Res) 2007;57(8):1439-1445.
Edition:
- Fourth Edition