Disclaimer: The findings and conclusions in this chapter are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Arthritis and other rheumatic conditions (AORC) comprise over 100 diseases. What most of them have in common is that they cause pain, aching, stiffness or swelling in or around a joint.
Definitions
Defining AORC to assess the burden in a population requires considering both what is important to measure and what data sources are available, such as population surveys and administrative data. Complicating any definition is the 100+ conditions that comprise what is generally thought of as “arthritis.” Furthermore, population measures need to be relatively simple and perhaps different from definitions used in clinical practice, where there is the luxury of having a medical history, physical examination, and laboratory and radiographic data. The Centers for Diseases Control and Prevention (CDC) Arthritis Program has worked with other organizations to develop case definitions, based on the best available expertise, that allow many measures of population burden to be addressed in a consistent way.1
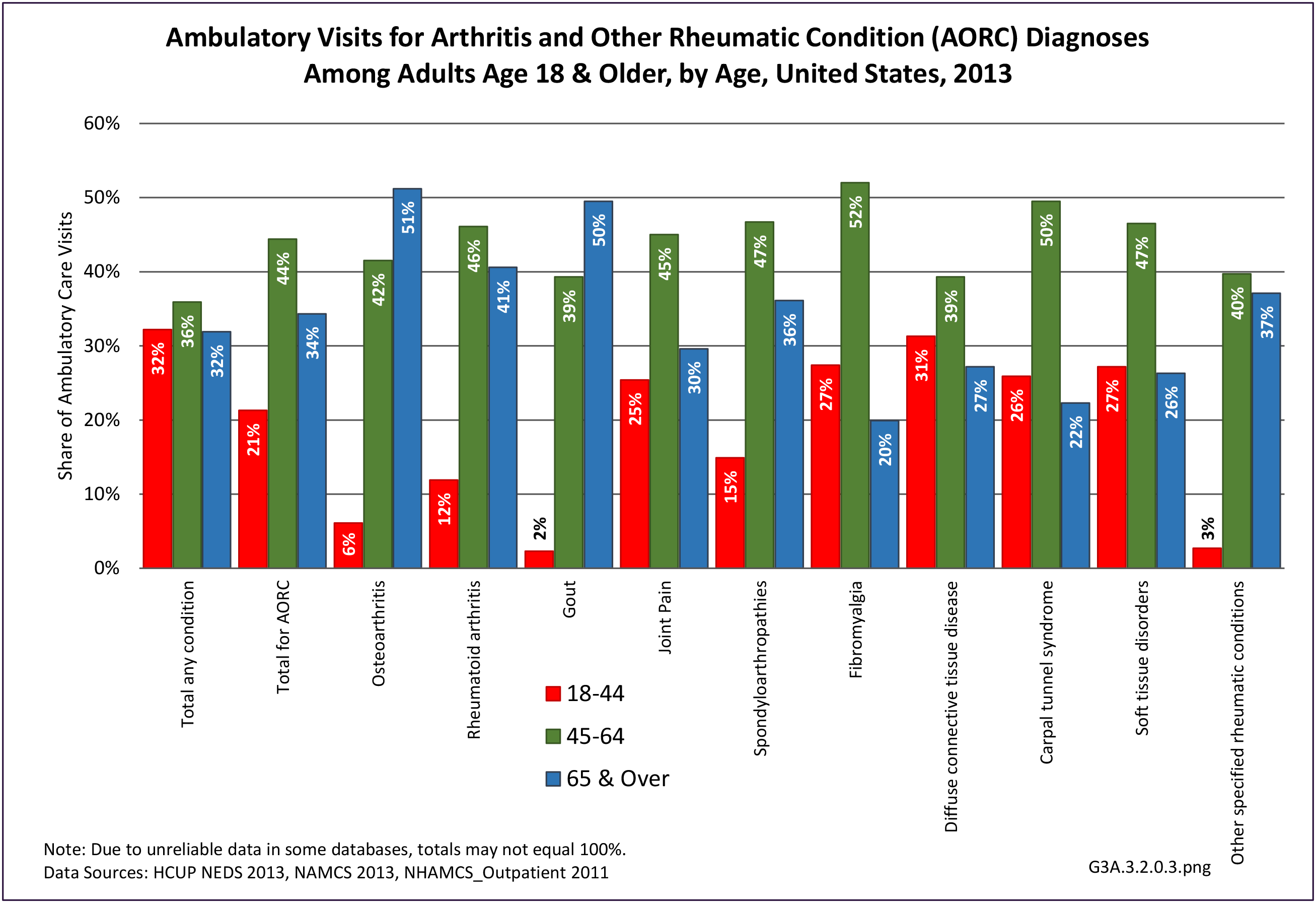
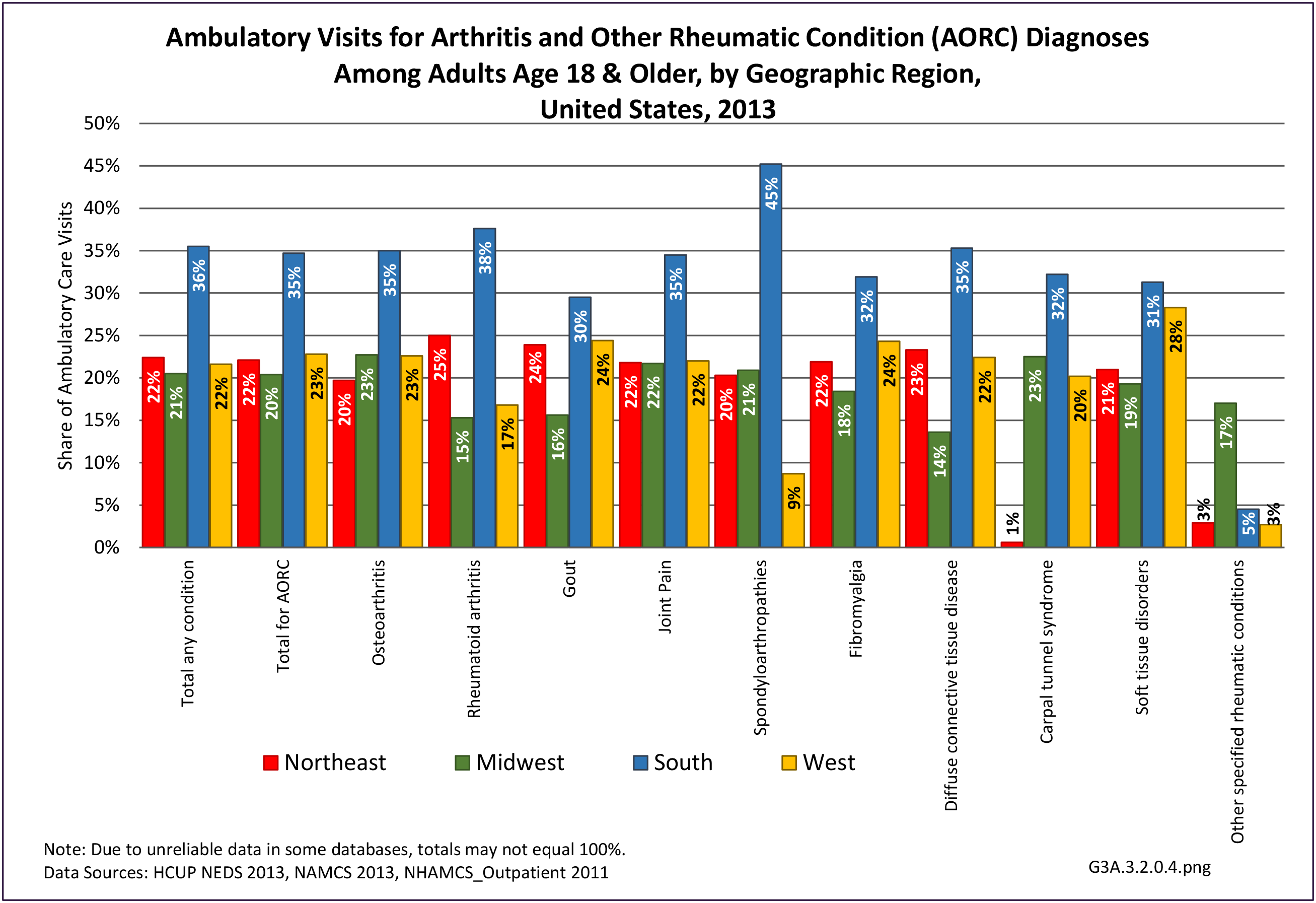
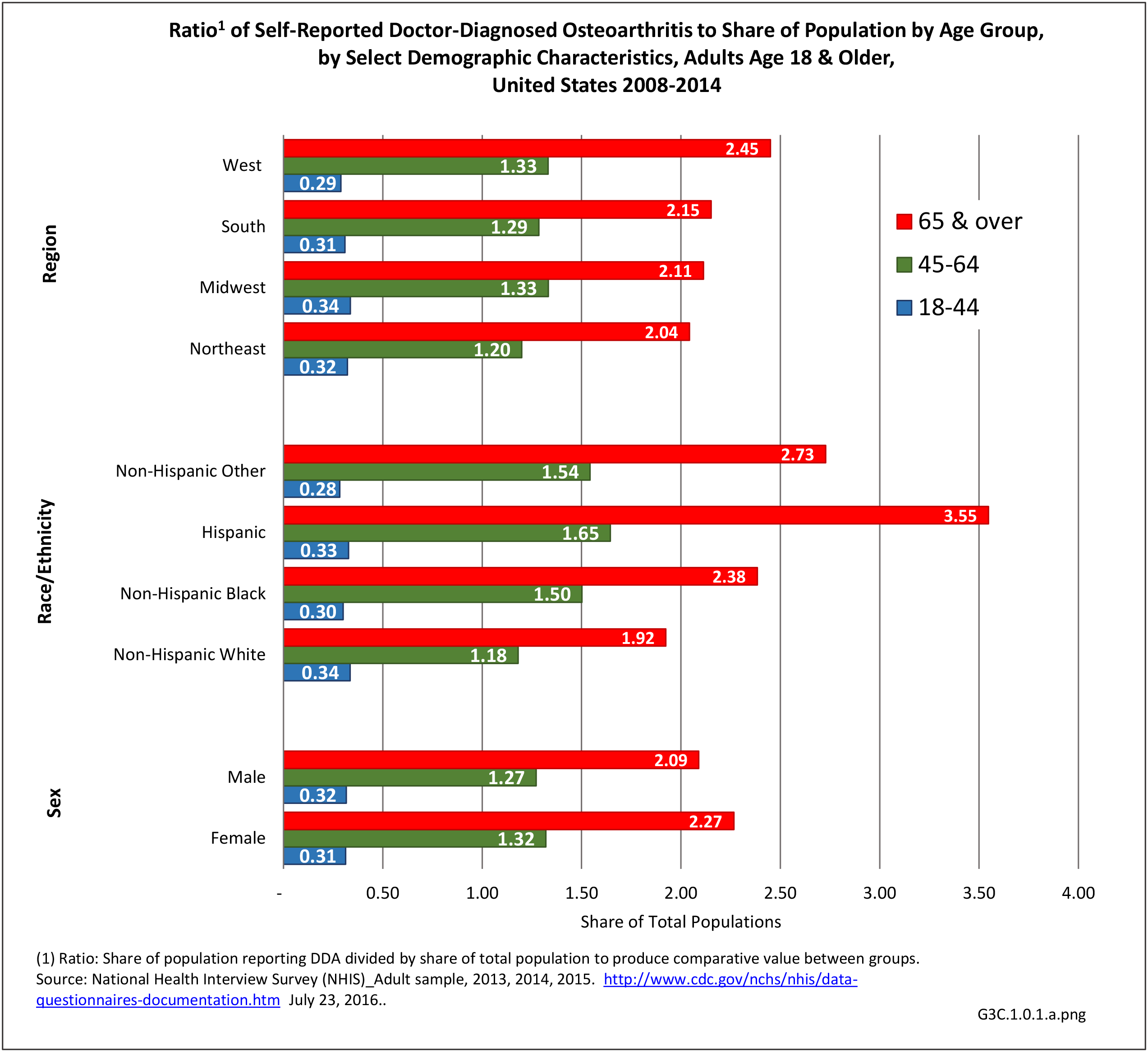
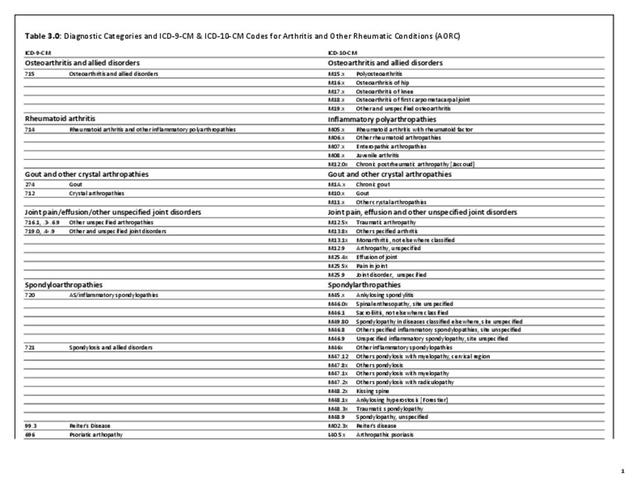
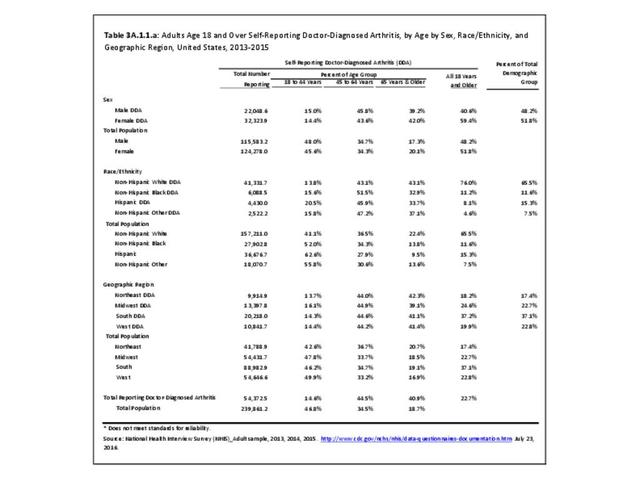
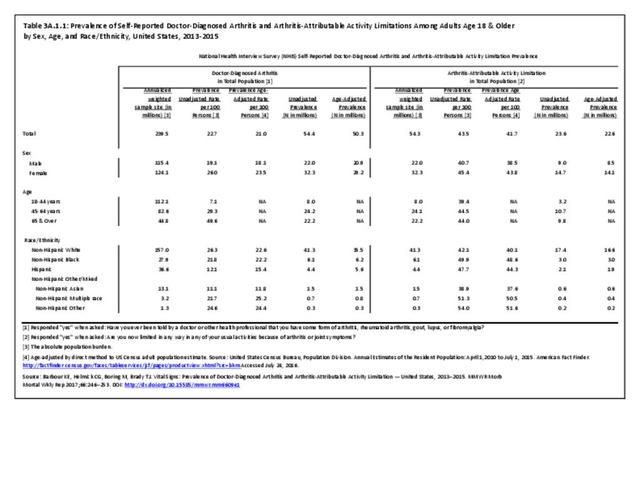
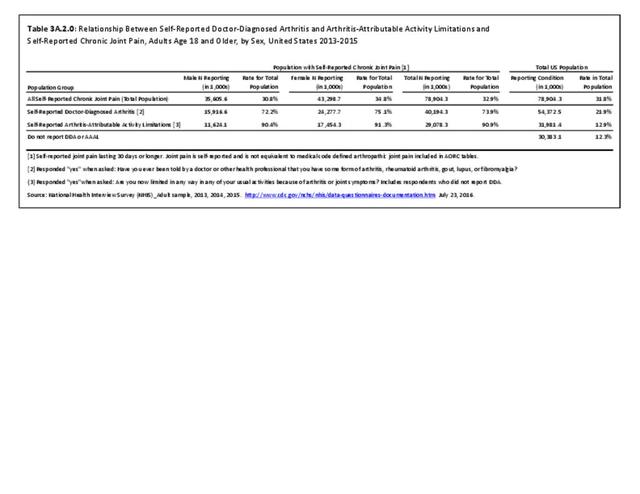
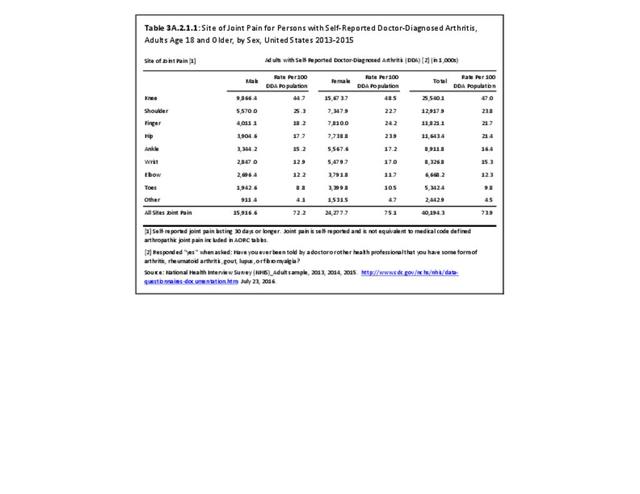
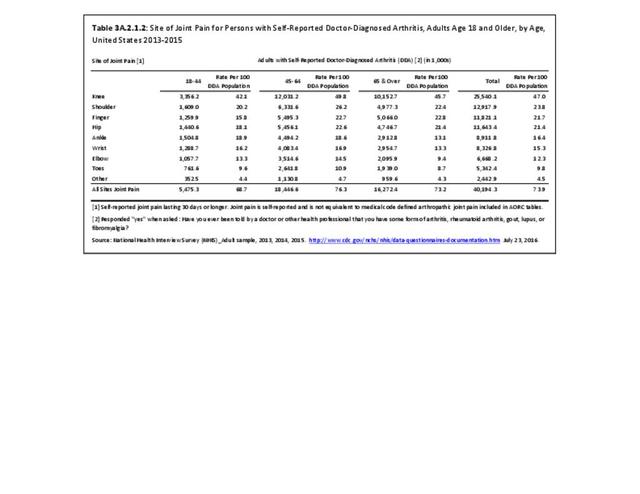
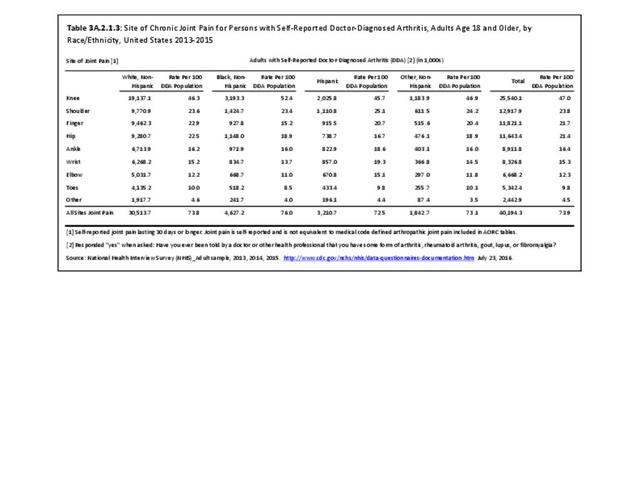
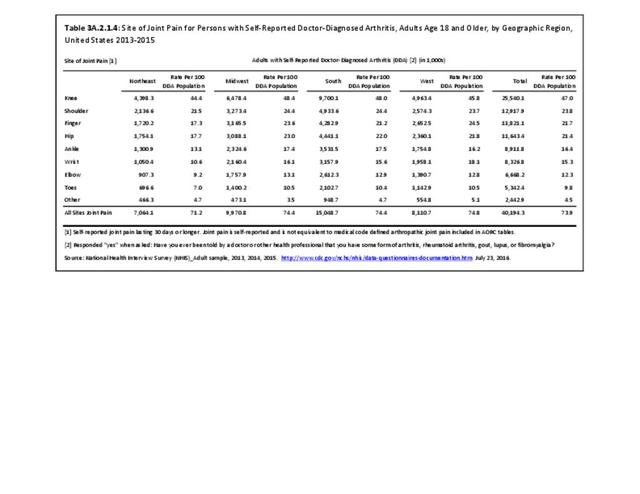
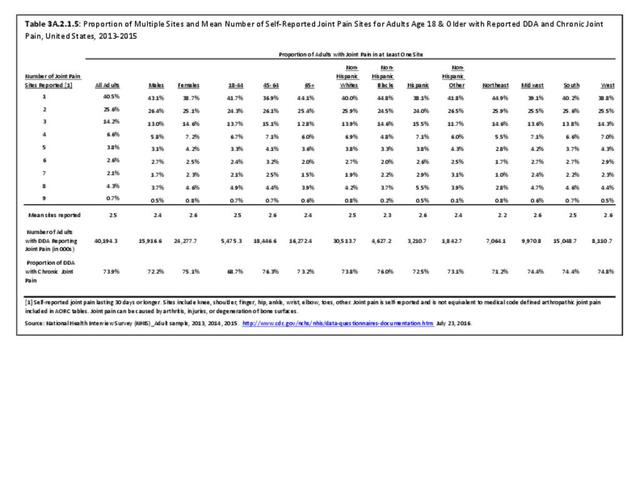
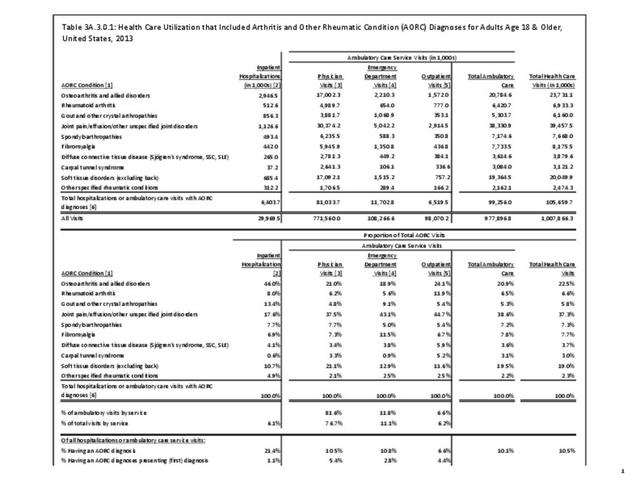
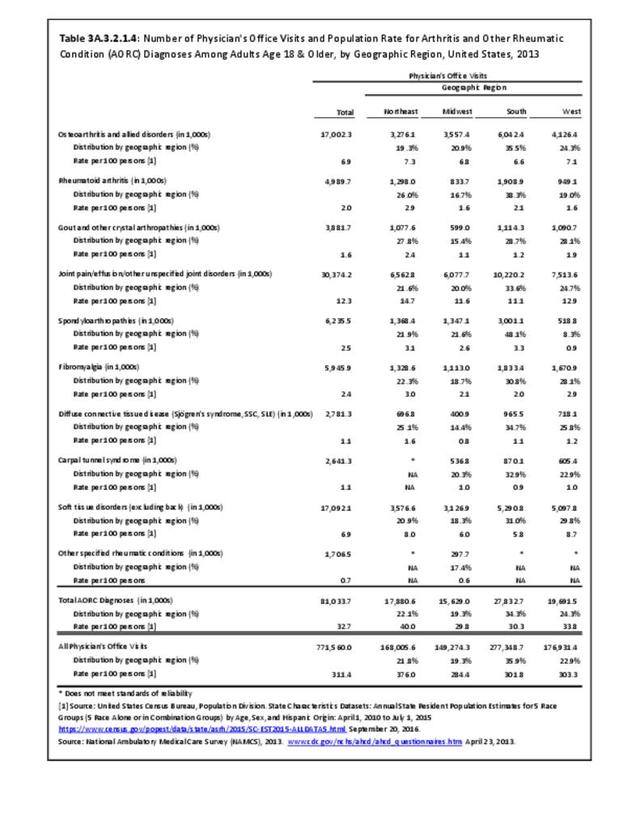
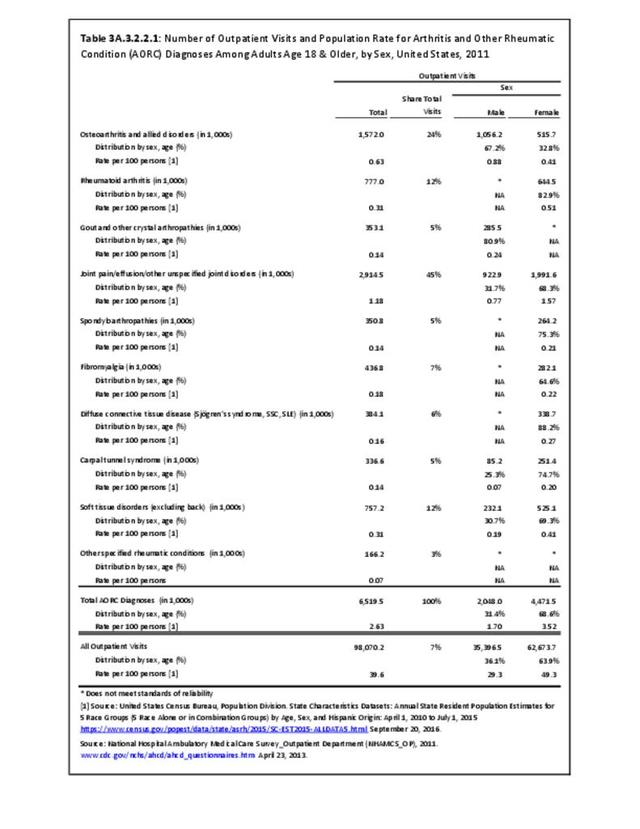
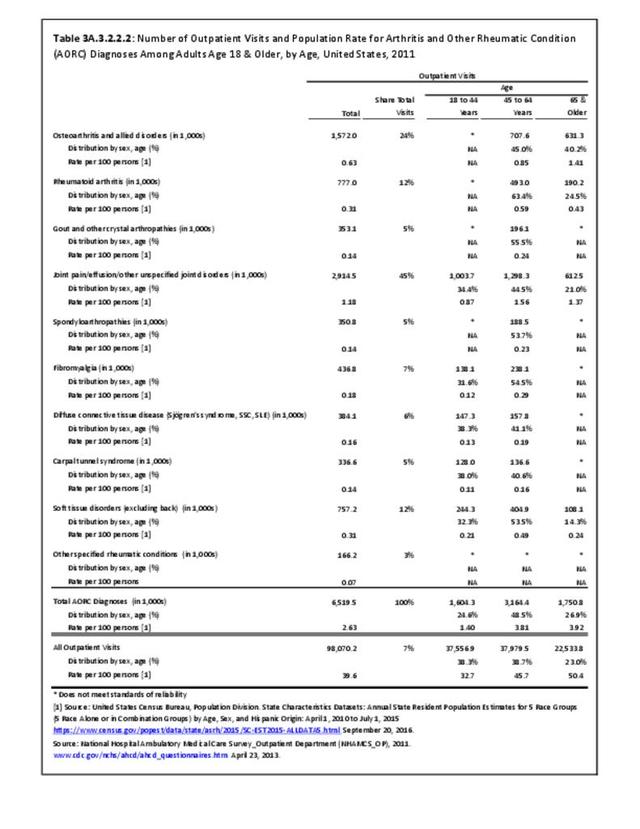
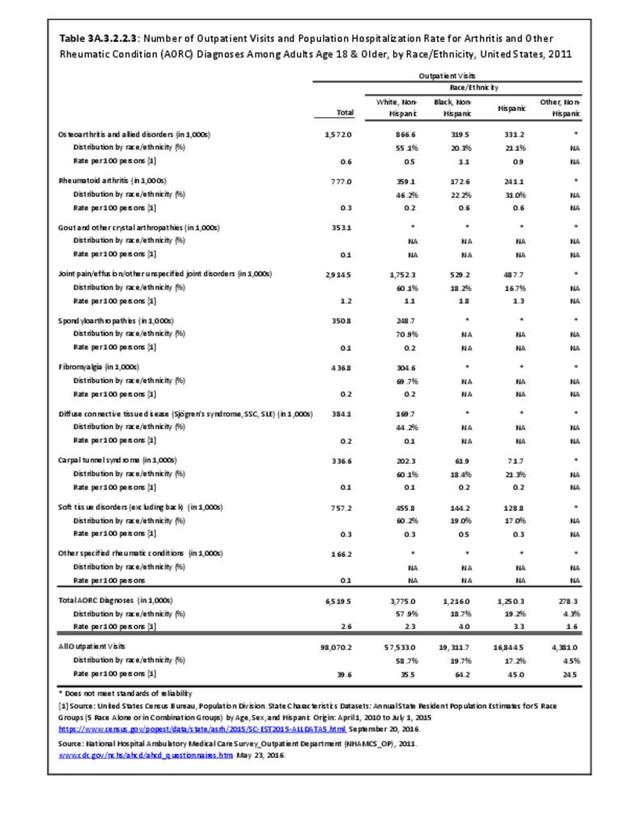
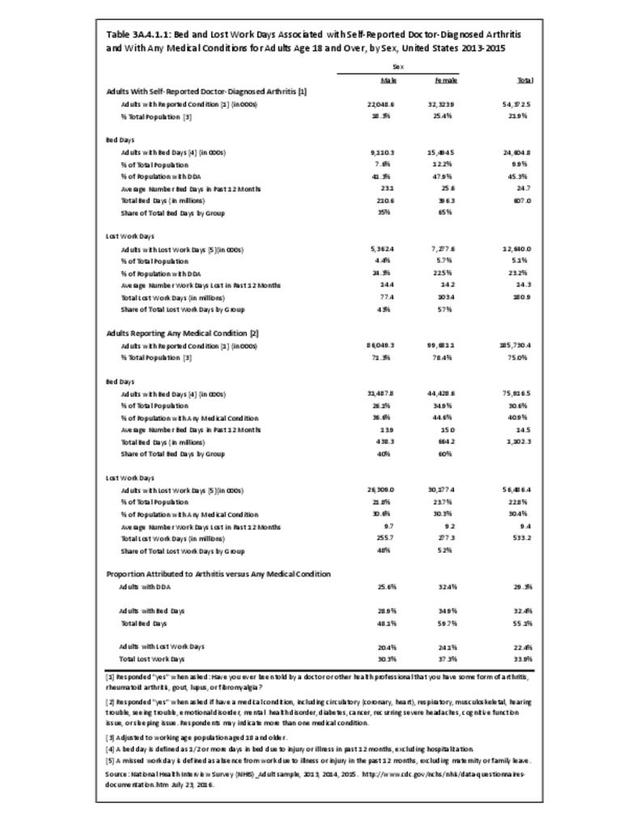
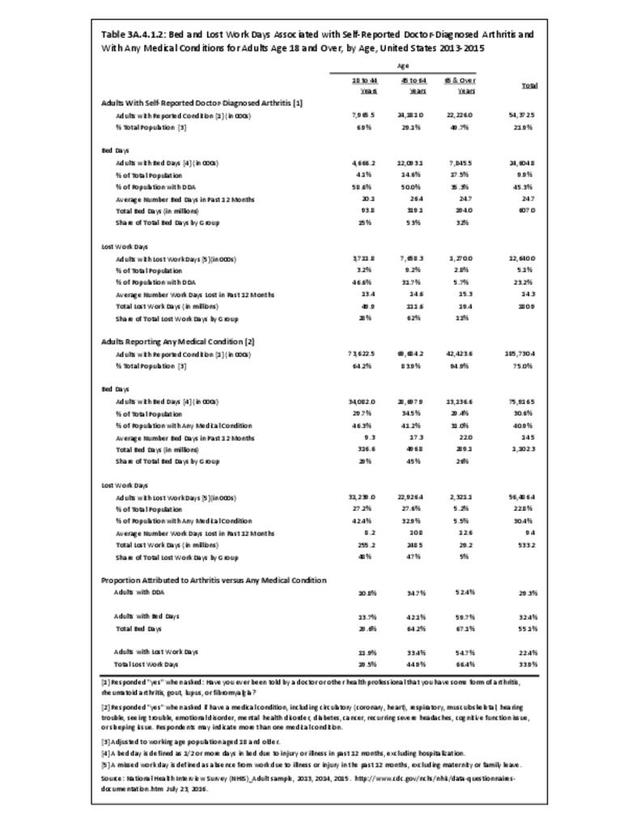
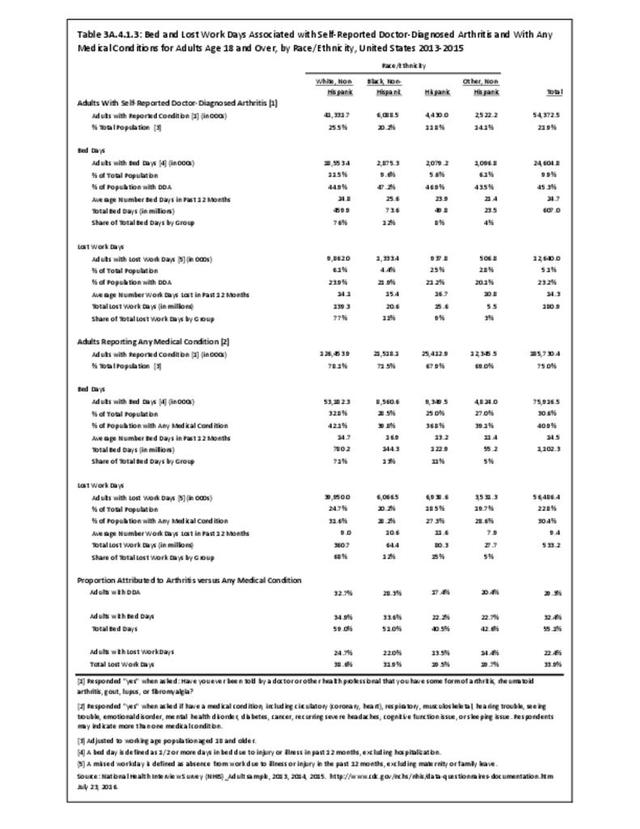
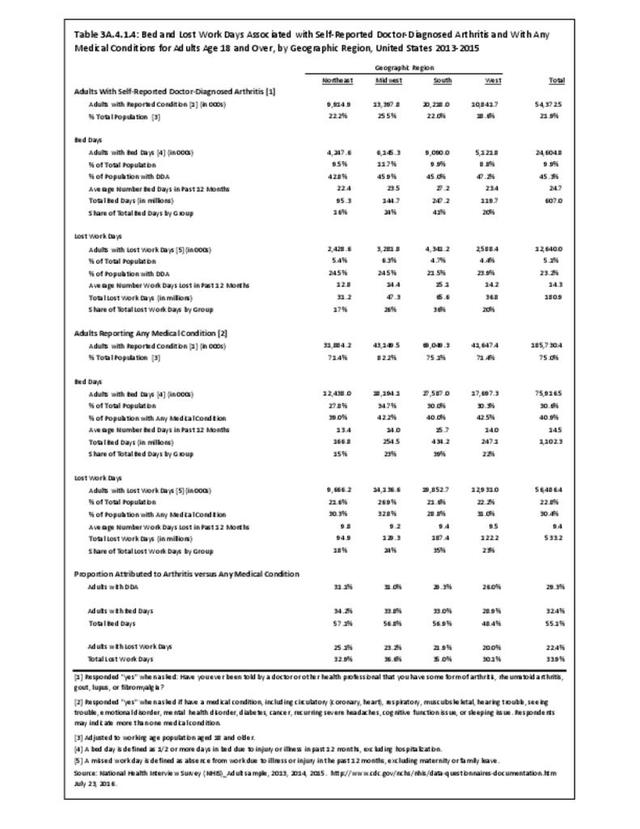
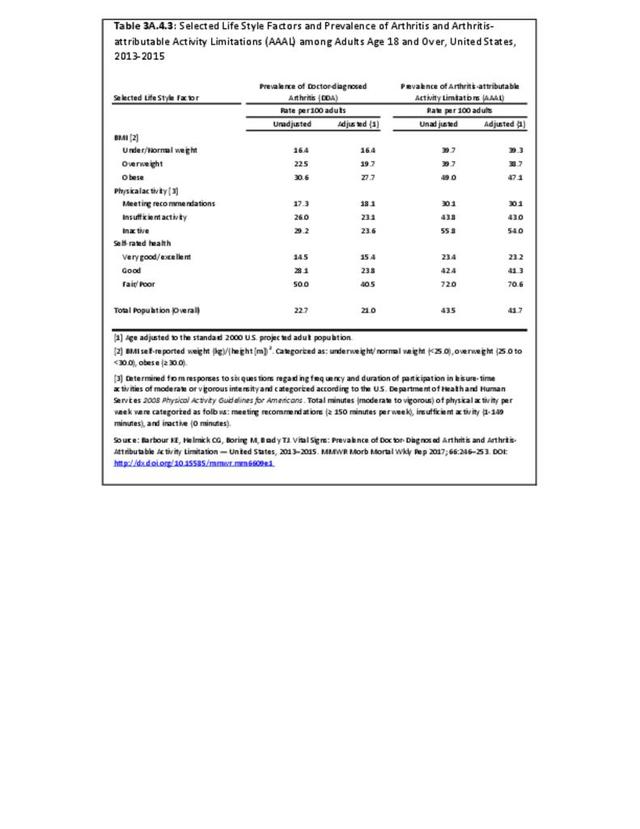
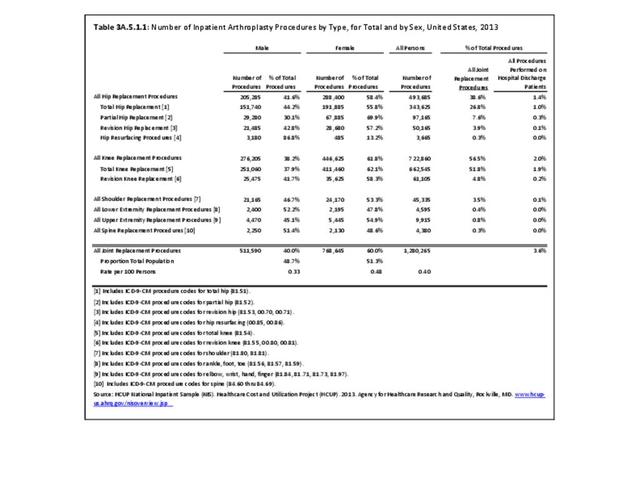
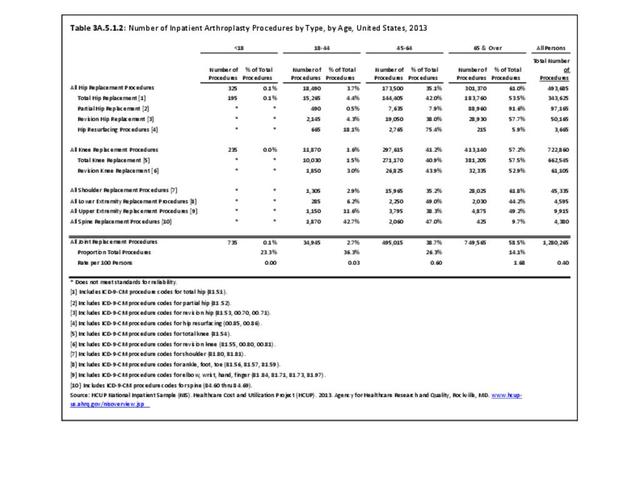
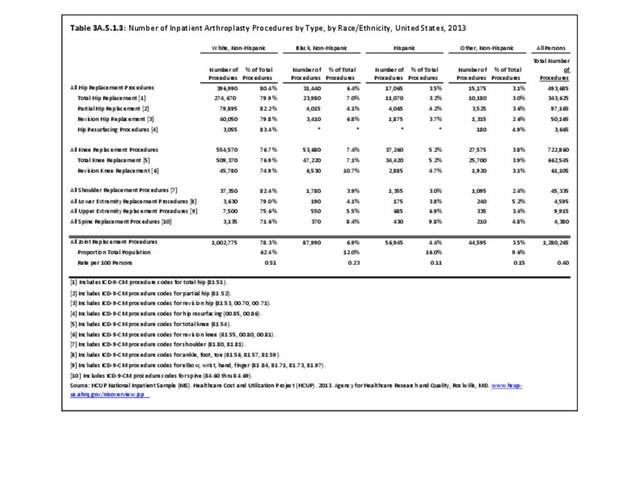
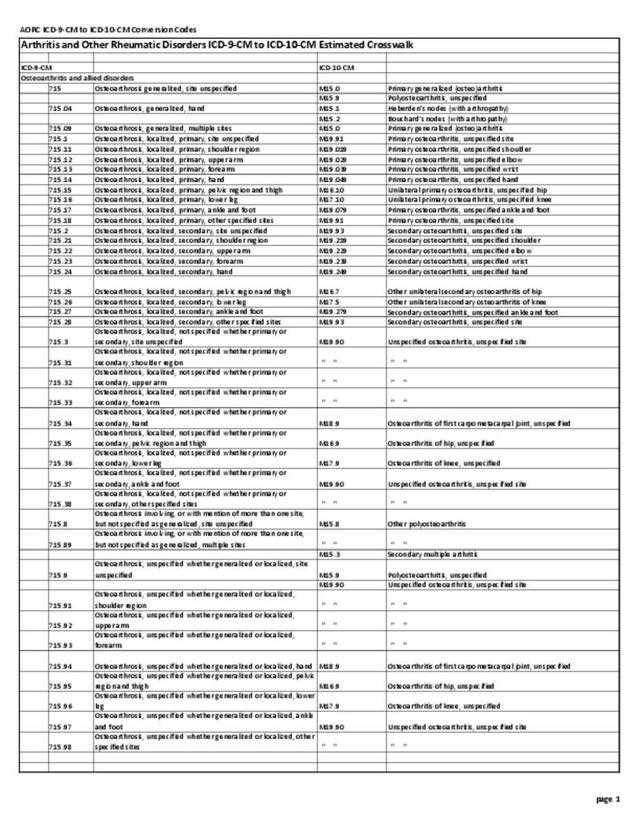
For self-reported population surveys, doctor-diagnosed arthritis (DDA) is defined as a “yes” answer to the question “Have you EVER been told by a doctor or other health professional that you have some form of arthritis, rheumatoid arthritis, gout, lupus, or fibromyalgia?” This measure aims to capture most of the major categories of arthritis and is considered valid for surveillance purposes of estimating population prevalence.2 For data sources using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes, arthritis and other rheumatic conditions (AORC) has been defined by the National Arthritis Data Workgroup using those codes, and further divided into ten more specific subcategories defined in Arthritis and Joint Pain Codes. Both definitions were designed to exclude or minimize other major categories of musculoskeletal disease, such as osteoporosis and generic chronic back pain, even though some chronic back pain is due to arthritis. DDA is likely better for estimating what is happening in the population at large because arthritis may not be mentioned or recorded at healthcare system encounters that are typically more focused on other conditions (e.g., diabetes, heart disease). However, even with the latter limitation, AORC is likely better for estimating what is happening in the healthcare system.
A recent review of relevant data sources considers the strengths and limitations of each of the different case definitions. Using DDA criteria, four databases defined prevalence within 3 percentage points, while using ICD-9-CM criteria they had a 5 percentage point spread. This study highlights the difficulty of applying a single number for estimating prevalence of AORC and the need to consider the purpose, design, measurement methods, and statistical precision of the data source being used.3
- 1. http://www.cdc.gov/arthritis/data_statistics/case_definition.htm
- 2. Sacks JJ, Harrold LR, Helmick CG, Gurwitz JH, Emani S, Yood RA. Validation of a surveillance case definition for arthritis. J Rheumatology 2005: 32(2):340-7.
- 3. Murphy LB, Cisternas MG, Greenlund KJ, et.al. Defining arthritis for public health surveillance: methods and estimates in four US population health surveys. Arthritis Care Res 2017;69(3):356-367.
Edition:
- Fourth Edition