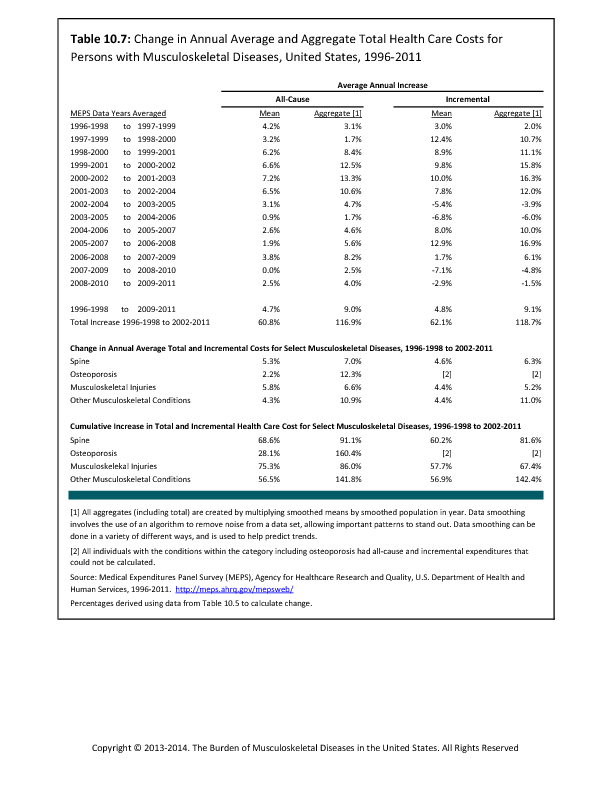
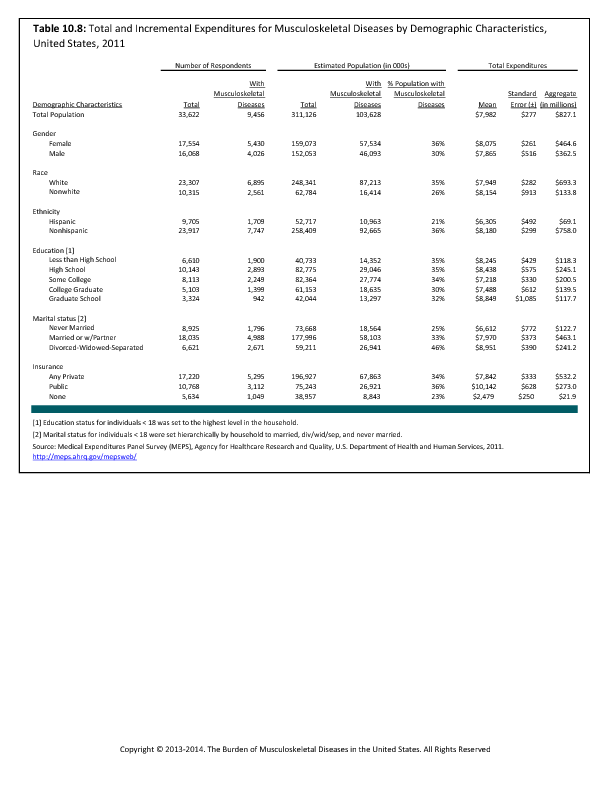
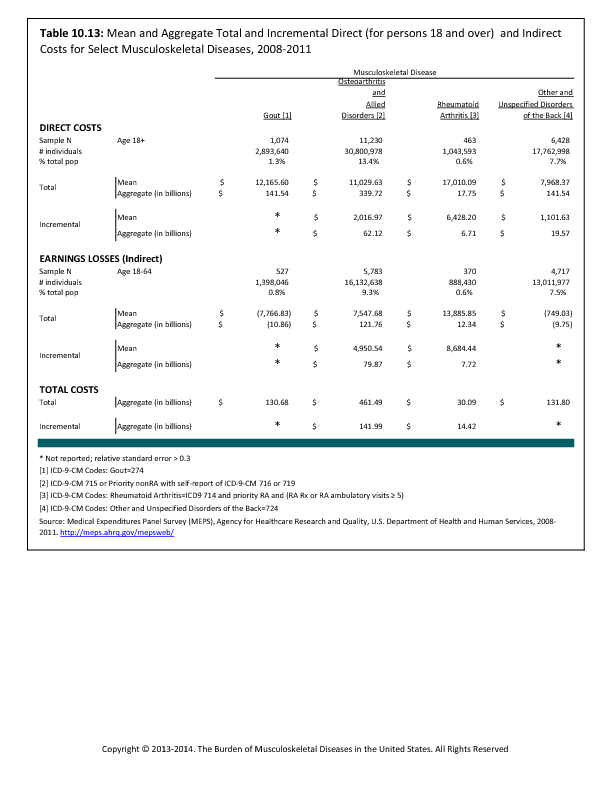
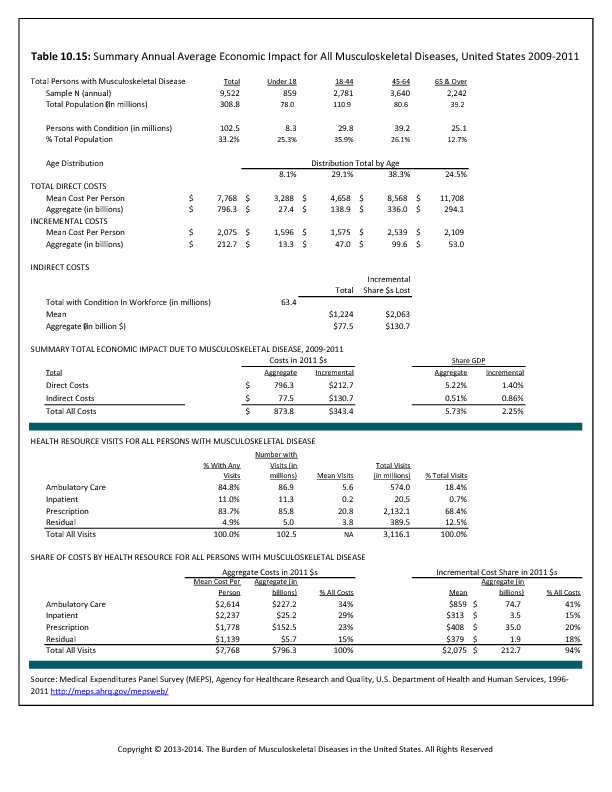
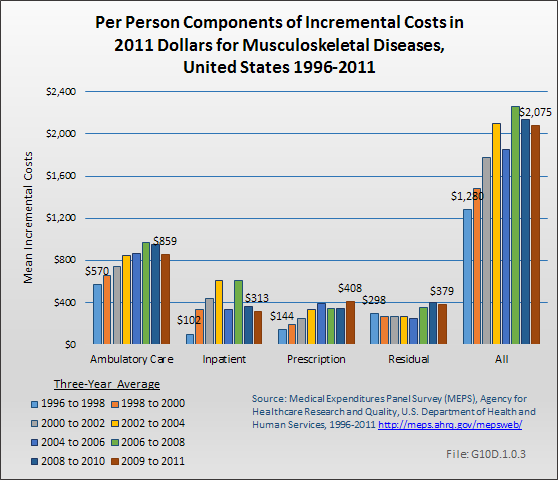
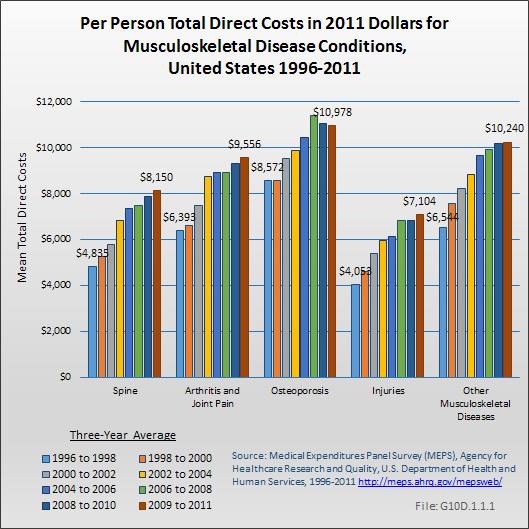
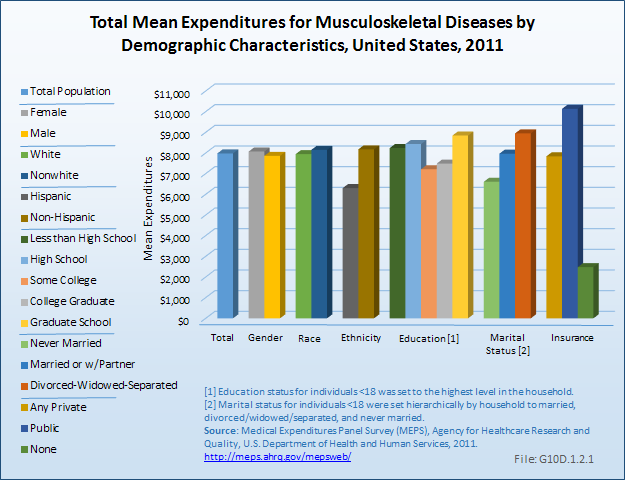
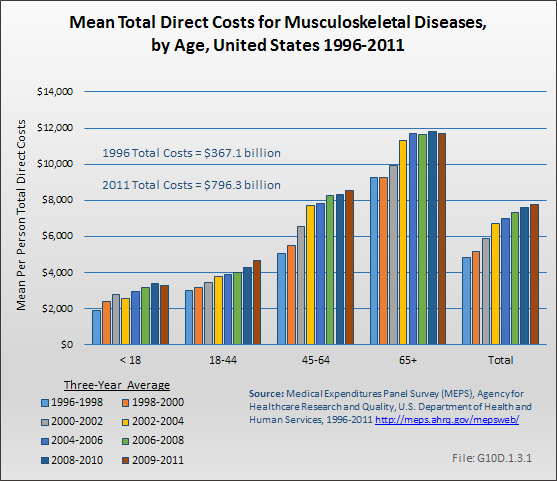
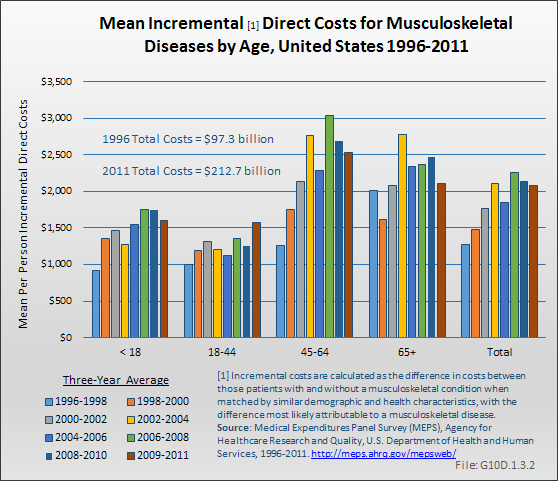
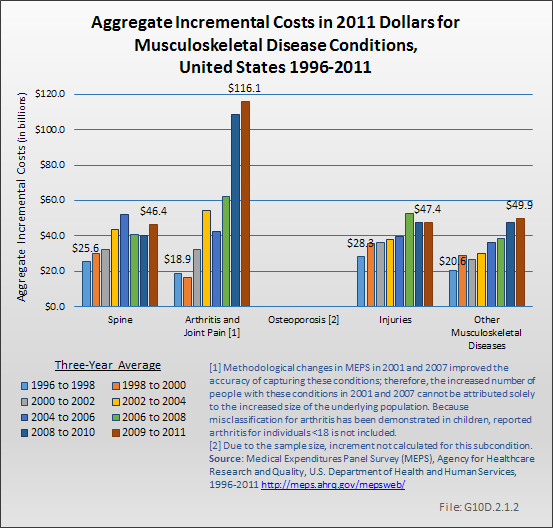
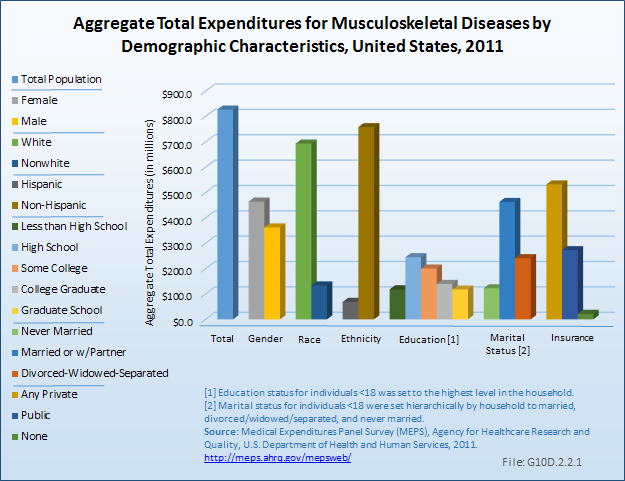
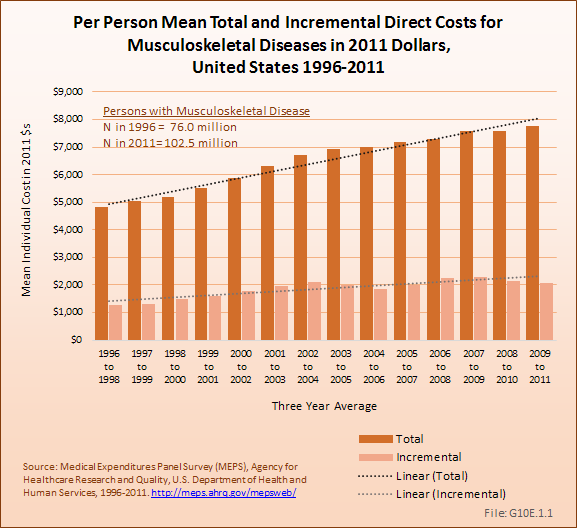
Economic cost for musculoskeletal-related health care diseases presented in this book are based on data from the Medical Expenditures Panel Survey (MEPS) using a methodology developed by the principal author and colleagues at the US Centers for Disease Control (CDC).1,2,3,4,5 The MEPS is a comprehensive data source designed for cost of illness studies.6,7,8,9 The MEPS uses a complex multistage probability sample of the US population and queries this sample three times annually about their medical conditions, health care utilization, and employment status, and provides information on the charges and expenditures associated with medical utilization. The authors use expenditure information to produce two types of cost estimates. The first, total cost, is an indication of all medical care costs and earnings losses incurred by persons with a musculoskeletal disease, regardless of the condition for which the cost was incurred. The second, incremental cost, is an estimate of the magnitude of cost that would be incurred beyond those experienced by persons of similar demographic and health characteristics but who do not have one or more musculoskeletal disease. Cost estimates are produced as the mean per-person medical care cost and as the aggregate, or sum of mean costs overall, associated with all persons with musculoskeletal diseases.
Early editions of this book based estimates of the economic impact of musculoskeletal diseases on the Rice cost of illness methodology.10,11 The Rice model utilized the National Hospital Discharge Survey (NHDS) and other available national health care data sources such as the National Health Interview Survey.12 All costs associated with hospitalizations or treatments for persons with a musculoskeletal disease listed as the primary, or first, diagnosis were included in the model. The Rice model defines direct cost as those associated with all components of medical care (ie, inpatient and outpatient care, medications, devices, and costs associated with procuring medical care), and indirect cost such as those associated with wage loss due to morbidity or mortality, plus an estimate of intangible costs.
In the Rice model, mortality accounted for 7% of total indirect medical cost for all conditions. The MEPS data do not provide a comparable method for calculating wage loss associated with mortality. Hence, total cost presented here represents an under-count by a similar percentage. Because musculoskeletal diseases have a smaller impact on mortality than most other major categories of illness, the under-count will be an unknown, but smaller, percentage.
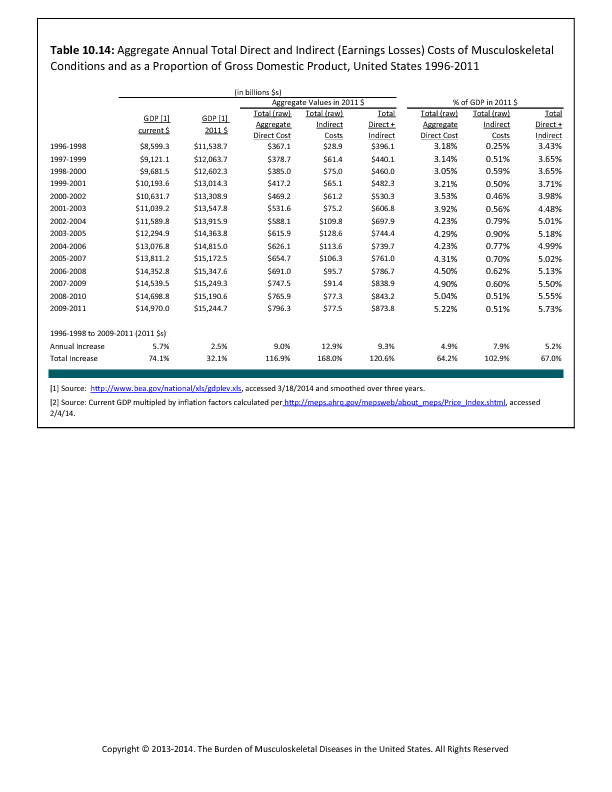
Comparing total cost for 1995 (the last year that Rice updated her estimates)11 updated to 1996 terms (the first year for which MEPS data is available), and omitting cost associated with mortality, the current analysis results in $207 billion in total cost associated with musculoskeletal diseases using the Rice method and about $143 billion using the MEPS database. The difference may be due to allocating a higher proportion of diagnoses to the musculoskeletal classification in the Rice study. The difference suggests that inferring time changes between the Rice studies and those using MEPS should be done with caution.
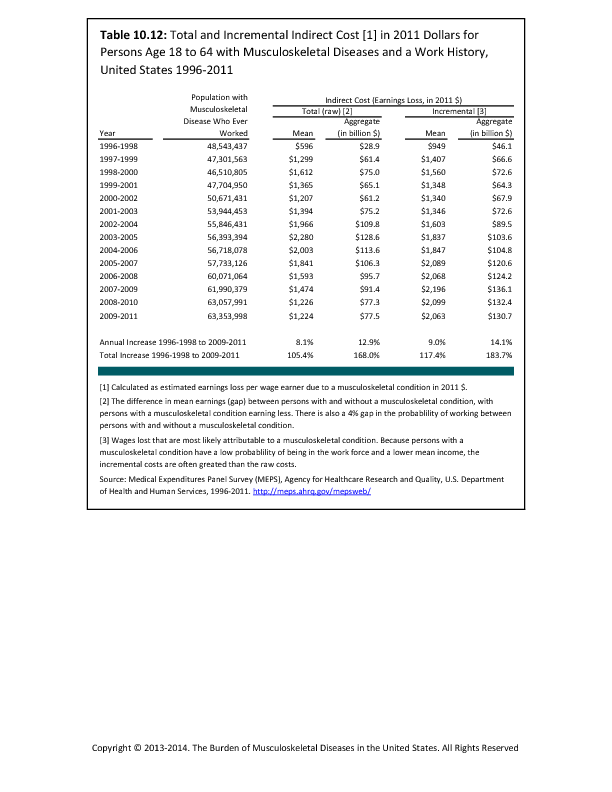
A series of papers provide a detailed description of the methods of estimating total and incremental direct and indirect cost of conditions, and outline the regression model used to adjust for differences of persons with and without musculoskeletal diseases due to demographic characteristics and health status.2,4 As in our previous work, we applied a two-stage model to estimate musculoskeletal condition-attributable costs for ambulatory, inpatient, prescription, and other expenditures, and a four-stage model for overall expenditures. However, the present analysis differs from prior analysis due to the use of a generalized linear model with a gamma distribution and a log-link, as opposed to a log transformation with a smearing estimate applied to back-transformed predicted values, in the stages predicting costs among individuals with any positive expenditures.
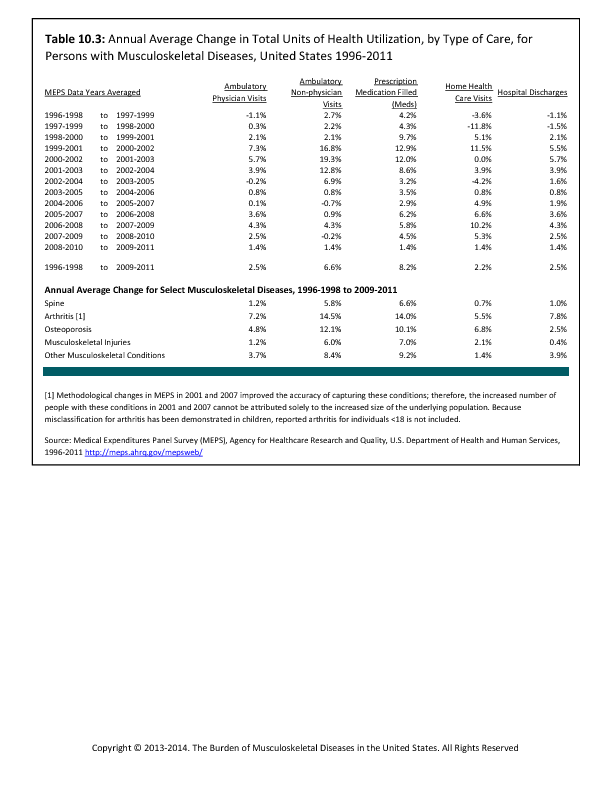
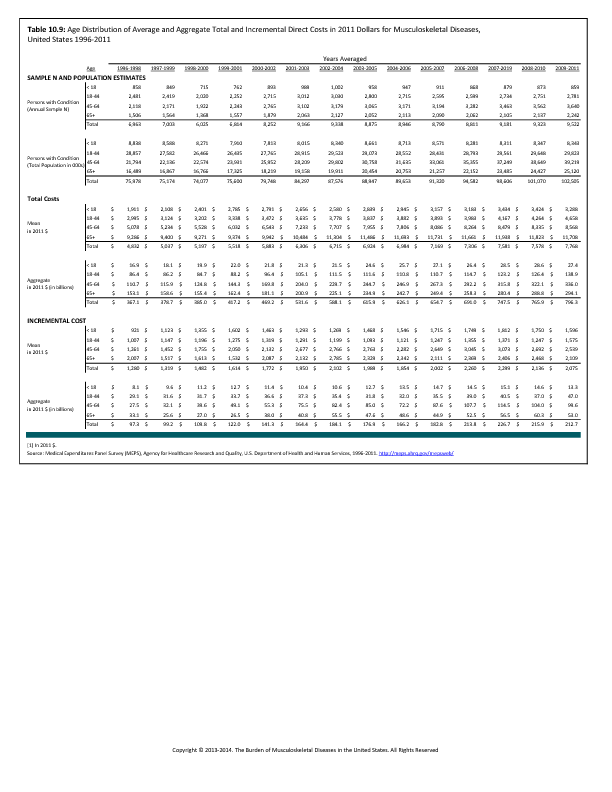
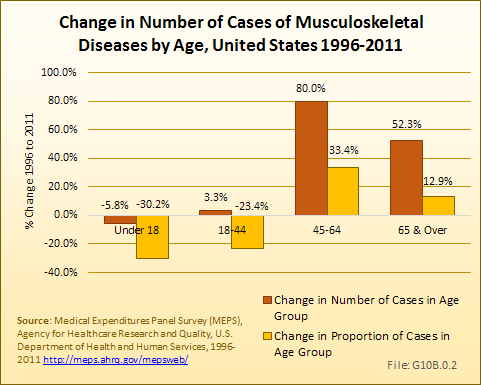
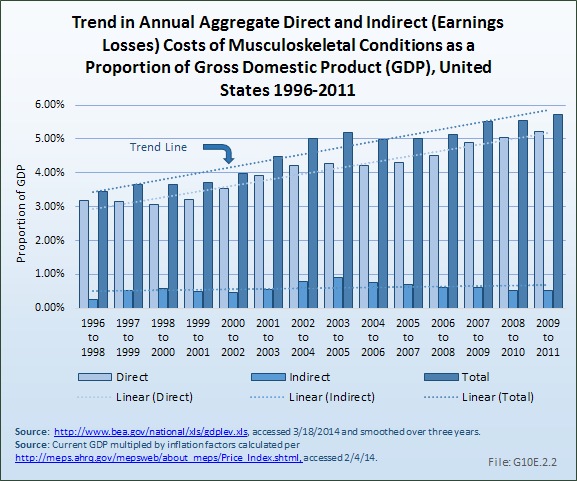
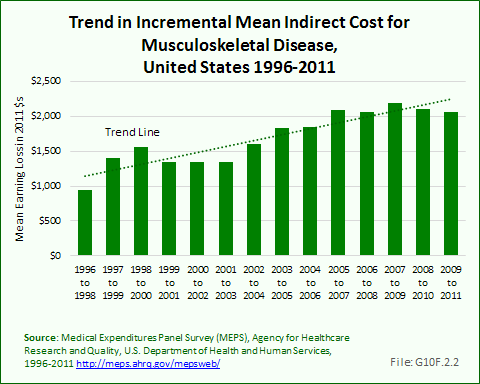
Although generally prevalence and cost associated with musculoskeletal diseases increase over time, sampling variability in the MEPS does not reflect this in each successive year. The impact of sampling variability is partially mitigated by smoothing, or averaging, data across 3-year periods.
- 1. Cisternas MG, Murphy LB, Yelin EH, Foreman AJ, Pasta DJ, Helmick CG: Trends in medical care expenditures of US adults with arthritis and other rheumatic conditions 1997 to 2005. J Rheumatol 2009;36(11):2531-2538. Epub 2009 Oct 1.
- 2. Yelin E, Cisternas M, Pasta D, et al: Medical care expenditures and earnings losses of persons with arthritis and other rheumatic conditions in the United States in 1997: Total and incremental estimates. Arthritis Rheum 2004;50(7):2317-2326.
- 3. Yelin E, Herrndorf A, Trupin L, Sonneborn D: A national study of medical care expenditures for musculoskeletal conditions: The impact of health insurance and managed care. Arthritis Rheum 2001;44:1160-1169.
- 4. Yelin E, Murphy L, Cisternas MG, et al: Medical care expenditures and earnings losses among persons with arthritis and other rheumatic conditions in 2003, and comparisons with 1997. Arthritis Rheum 2007;56(5):1397-1407.
- 5. Yelin E, Trupin L, Cisternas M: Direct and Indirect Costs of Musculoskeletal Conditions in 1997: Absolute and Incremental Estimates. Atlanta, GA, Centers for Disease Control, 2002.
- 6. Cohen J, Monheit A, Beauregard K. The Medical Expenditure Panel Survey: A national information resource. Inquiry 1996-1997;33:373-389.
- 7. Cohen S: Sample Design of the 1996 Medical Expenditure Panel Survey Household Component. Washington, DC, Agency for Health Care Policy and Research: US Department of Health and Human Services, 1997.
- 8. Cohen S: Sample Design of the 1997 Medical Expenditure Panel Survey Household Component. Washington, DC, Agency for Health Care Policy and Research: US Department of Health and Human Services, 2000.
- 9. Cohen S, DiGaetano R, Goksel H: Estimation Procedures in the 1996 Medical Expenditure Panel Survey Household Component. Washington, DC, Agency for Health Care Policy and Research: US Department of Health and Human Services, 1999.
- 10. Rice D: Cost of musculoskeletal conditions, in Praemer A, Furner S, Rice D, eds: Musculoskeletal Conditions in the US. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1992.
- 11. Rice D: Cost of musculoskeletal conditions, in Praemer A, Furner S, Rice D, eds: Musculoskeletal Conditions in the US, ed 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1999.
- 12. Yelin E, Katz P: Labor force participation among persons with musculoskeletal conditions, 1970-1987: National estimates derived from a series of cross-sections. Arthritis Rheum 1991;34:1361-1370.
Edition:
- 2014















 Download as CSV
Download as CSV