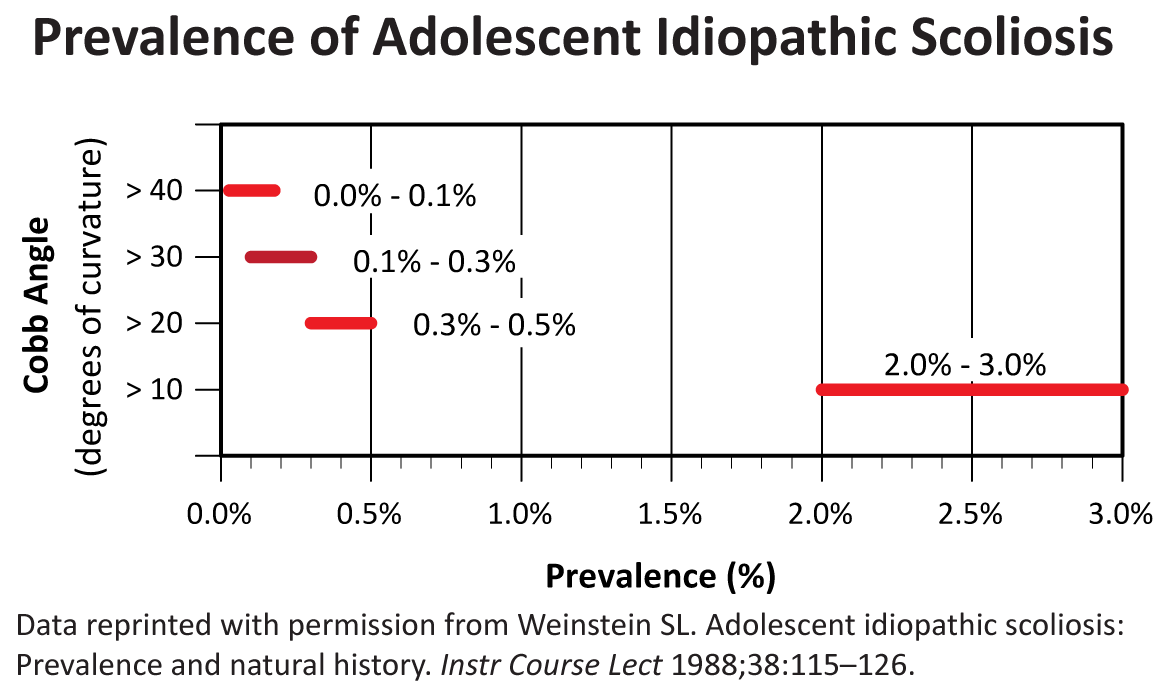
According to the Scoliosis Research Society (SRS), idiopathic scoliosis is diagnosed when a patient has asymmetry on forward bending combined with a curve of at least 10°.1 By this definition, the prevalence of adolescent idiopathic scoliosis in children from 10 to 16 years of age is 2% to3%. Though the male-to-female ratio for smaller curves is about equal, larger curves seem to be more common in females. Similar results were found in a study conducted in 1985, where 29,195 children were screened for idiopathic scoliosis.2
Several studies have investigated the natural history and natural course of curve progression in adolescent idiopathic scoliosis. All report the strongest predictive factors in the development of idiopathic scoliosis are age, magnitude of curve, and gender.3,4,5,6,7 Girls are more likely to have adolescent idiopathic scoliosis than boys, and some studies report the onset is earlier in girls than boys. A factor highly correlated with curve progression is age at diagnosis; patients diagnosed at a younger age have a greater risk of curve progression. However, those diagnosed at a younger age seem to have a more favorable response to milder forms of treatment, which supports the practice of school screening to detect and lead to earlier diagnosis for those children with a smaller degree of curvature.
Treatment decisions for individuals with adolescent idiopathic scoliosis are made based on location, shape, pattern, and cause of the curve. The treatment choice is also a function of the patient’s future growth potential. Treatment choices include observation, bracing, and surgery. Observation is usually reserved for patients who have curves ≤25°. Bracing, which is used to stop curve progression (rather than for lasting correction of the curve), is usually used for patients who have curves ≥25° and who are still growing. Surgery is generally used for patients with curves ≥45°.
- 1. Lonstein J: Scoliosis: Surgical versus nonsurgical treatment. Clin Ortho Relat Res 2006;443:248-259.
- 2. Morais T, Bernier M, Turcotte F: Age- and sex-specific prevalence of scoliosis and the value of school screening programs. Am J Public Health Nations Health 1985;75:1377-1380.
- 3. Bunnell W: Spinal deformity. Pediatr Clin North Am 1986;33:1475-1487.
- 4. Weinstein S: Idiopathic scoliosis: Natural history. Spine 1986;11:780-783.
- 5. Karol LA, Johnston CE 2nd, Browne RH, Madison M: Progression of the curve in boys who have idiopathic scoliosis. J Bone Joint Surg Am 1993;75:1804-1810.
- 6. Porter SB, Blount BW: Pseudotumor of infancy and congenital mascular torticollis. Am Fam Physician 1995;52:1731-1736.
- 7. Willner S: Continuous screening and treatment of teenage scoliosis is recommended. Lakartidningen 1994;91:22.
Edition:
- 2014










 Download as CSV
Download as CSV